Managing Medical and Obstetric Emergencies and Trauma
Здесь есть возможность читать онлайн «Managing Medical and Obstetric Emergencies and Trauma» — ознакомительный отрывок электронной книги совершенно бесплатно, а после прочтения отрывка купить полную версию. В некоторых случаях можно слушать аудио, скачать через торрент в формате fb2 и присутствует краткое содержание. Жанр: unrecognised, на английском языке. Описание произведения, (предисловие) а так же отзывы посетителей доступны на портале библиотеки ЛибКат.
- Название:Managing Medical and Obstetric Emergencies and Trauma
- Автор:
- Жанр:
- Год:неизвестен
- ISBN:нет данных
- Рейтинг книги:3 / 5. Голосов: 1
-
Избранное:Добавить в избранное
- Отзывы:
-
Ваша оценка:
Managing Medical and Obstetric Emergencies and Trauma: краткое содержание, описание и аннотация
Предлагаем к чтению аннотацию, описание, краткое содержание или предисловие (зависит от того, что написал сам автор книги «Managing Medical and Obstetric Emergencies and Trauma»). Если вы не нашли необходимую информацию о книге — напишите в комментариях, мы постараемся отыскать её.
MANAGING MEDICAL AND OBSTETRIC EMERGENCIES AND TRAUMA A PRACTICAL APPROACH
provides an evidence-based, structured approach to the recognition and treatment of emergencies in pregnancy. This contemporary resource provides step-by-step guidance on the knowledge, practical skills and procedures required to improve outcomes for the mother and fetus. Now in its fourth edition, the text fully aligns with the mMOET course, and has been extensively reviewed and revised throughout. Lessons learned from mortality reports and national guidelines underpin the new material. This edition includes: New chapters on cardiac disease, neurological emergencies and human factors An update for obstetric teams treating pregnant trauma patients in line with modern trauma management Revised algorithms and new illustrations
is a vital source of practical information presented as a systematic approach to prepare the obstetric team: obstetricians, midwives, anaesthetists and emergency physicians. The Advanced Life Support Group (ALSG)
Managing Medical and Obstetric Emergencies and Trauma — читать онлайн ознакомительный отрывок
Ниже представлен текст книги, разбитый по страницам. Система сохранения места последней прочитанной страницы, позволяет с удобством читать онлайн бесплатно книгу «Managing Medical and Obstetric Emergencies and Trauma», без необходимости каждый раз заново искать на чём Вы остановились. Поставьте закладку, и сможете в любой момент перейти на страницу, на которой закончили чтение.
Интервал:
Закладка:
2 Knight M, Bunch K, Tuffnell D, et al. (eds), on behalf of MBRRACE‐UK. Saving Lives, Improving Mothers’ Care – Lessons Learned to Inform Maternity Care from the UK and Ireland Confidential Enquiries into Maternal Deaths and Morbidity 2015–17. Oxford: National Perinatal Epidemiology Unit, University of Oxford, 2019.
3 Knight M, Bunch K, Tuffnell D, et al. (eds), on behalf of MBRRACE‐UK. Saving Lives, Improving Mothers’ Care – Lessons learned to Inform Maternity Care from the UK and Ireland Confidential Enquiries into Maternal Deaths and Morbidity 2016–18. Oxford: National Perinatal Epidemiology Unit, University of Oxford, 2020.
CHAPTER 3 Structured approach to emergencies in the obstetric patient
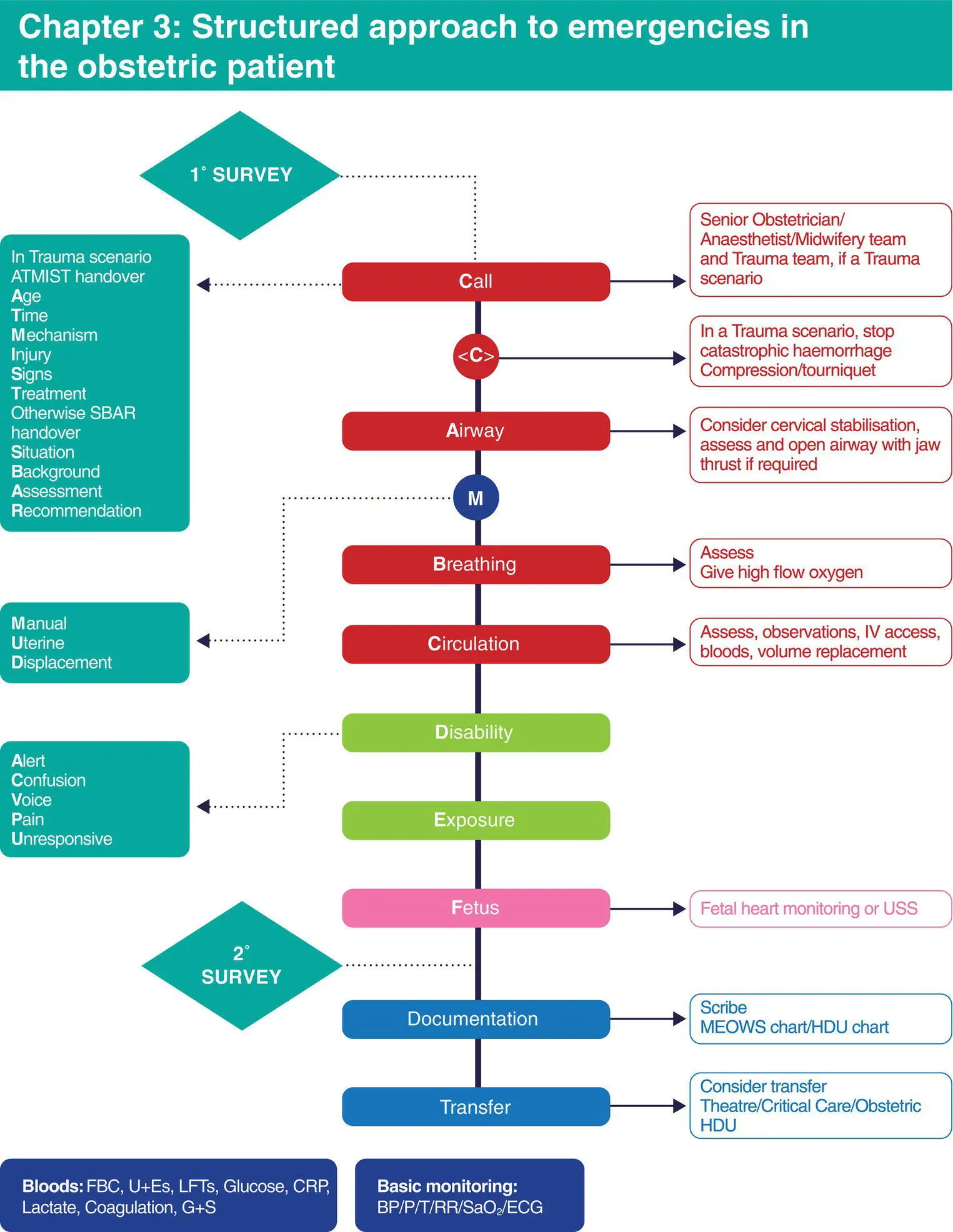
Algorithm 3.1 Structured approach to emergencies in the obstetric patient
Learning outcomes
After reading this chapter, you will be able to:
Identify the correct sequence to be followed in assessing and managing seriously ill or seriously injured patients
Outline the concept of the primary and secondary surveys
3.1 Introduction
The structured approach refers to the ‘ABCDE’ approach to life saving. The aim of the structured approach is to provide a system of assessment and management that is effective, and simple to remember, in the heat of an emergency. It can be applied to any patient with a threat to life, be that from illness or injury. Assessment is divided into primary survey and secondary survey. The approach is the same for all: adults, children, the elderly and pregnant women.
Primary survey
The system follows a simple ABCDE approach, with resuscitation taking place as problems are identified, i.e. a process of simultaneous evaluation and resuscitation.
The primary survey uncovers immediately life‐threatening problems by priority, i.e. in the order in which they will most quickly kill. The medical sequence in the ABCDE approach is that an Airway problem will kill the patient more quickly than a Breathing problem, which in turn will kill a patient more quickly than a Circulation problem, which in turn will kill a patient more quickly than a Disability (neurological) problem.
Airway
Assess whether the airway is open by look, listen and feel. If not open, proceed to open the airway using simple manoeuvres, such as head tilt and chin lift, followed by more complex actions (as detailed in Chapter 10) where necessary. Manoeuvres to secure the patient’s airway should not cause harm, or further harm, to the cervical spine. Therefore, if an injury to the cervical spine is suspected the cervical spine must be immobilised during airway care.
Breathing
Look, listen and feel for respiration, using supplementary oxygen and ventilatory support as required.
Circulation
Assess the circulation by checking perfusion, heart rate and blood pressure. Volume replacement and haemorrhage control may be needed (see Chapters 6and 8).
Disability
Assessment and support of the functioning of the neurological system including an assessment of conscious level (ACVPU), the pupils and a blood sugar.
Exposure
Adequately expose the patient to make a full assessment, taking care to avoid cooling and potential hypothermia by adjusting the environment.
3.2 Resuscitation
The resuscitation phase is carried out at the same time as the primary survey. Life‐threatening conditions are managed as they are identified. Do not move on to the next stage of the primary survey until a problem, once found, has been corrected. If the patient’s condition deteriorates, go back and reassess, starting again with ABCDE.
Secondary survey
The secondary survey is a comprehensive assessment, which takes place after life‐threatening problems have been found and treated (primary survey) and uncovers problems that are not immediately life threatening. Ensure a full history is taken using AMPLE as an aide memoire:
| A | Allergies |
| M | Medications |
| P | Past medical history, pregnancy issues |
| L | Last meal |
| E | Background to the illness/injury in terms of events and environment |
The secondary survey is performed once the patient is stable. The secondary survey might not take place until after surgery, if surgery has been necessary as part of the resuscitation phase. The secondary survey is a top‐to‐toe and back‐to‐front process, as follows:
Scalp and vault of skull
Face and base of skull
Neck and cervical spine
Chest
Abdomen
Pelvis
Remainder of spine and limbs
Neurological examination
Rectal and vaginal examinations, if indicated
Examination of wounds caused by injury. Note: do not remove foreign objects from penetrating wounds, they may be tamponading a bleeding vessel
If the Glasgow Coma Score has not been evaluated in the primary survey it should be performed during the secondary survey (see Chapter 19).
Assessment of the collapsed patient using the ABC approach
First, speak loudly to the patient. To prompt manual uterine displacement (MUD) early in the process of resuscitation, remember:
‘Hello, how are you Ms MUD?’
The response gives you several pieces of clinical information. To be able to respond verbally, the patient must have:
Circulating oxygenated blood (i.e. has not had a cardiopulmonary arrest)
A reasonably open airway
A reasonable tidal volume to phonate
Reasonable cerebral perfusion to comprehend and answer
If the patient does not respond then we cannot make the above assumptions.
Management of the apparently lifeless (unresponsive) patient
The approach to an apparently lifeless patient is the cardiopulmonary resuscitation (CPR) drill, which starts with opening the airway and assessing breathing, then proceeding to CPR as necessary (see Chapter 11for details).
Management of the seriously injured pregnant patient
In the seriously injured patient who has signs of life, the following approach is taken.
If possible receive the ATMIST handover from the pre‐hospital team and ensure left lateral tilt is ongoing or manually displace the uterus.
| A | Age and gestational age |
| T | Time of injury |
| M | Mechanism of injury |
| I | Injuries sustained or suspected |
| S | Signs and symptoms |
| T | Treatment given so far |
1 Primary survey and resuscitation: identify life‐threatening problems and deal with these problems as they are identified. In a multiply injured patient precedes ABCDE. is control of Catastrophic haemorrhage such as applying a tourniquet and compression bandage to an amputated limb.
2 Assess fetal well‐being and viability: may require delivery.
3 Secondary survey: top‐to‐toe, back‐to‐front examination.
4 Definitive care: specific management.
Continuous re‐evaluation is very important to identify new life‐threatening problems as they arise.
Monitoring (applied during primary survey)
Интервал:
Закладка:
Похожие книги на «Managing Medical and Obstetric Emergencies and Trauma»
Представляем Вашему вниманию похожие книги на «Managing Medical and Obstetric Emergencies and Trauma» списком для выбора. Мы отобрали схожую по названию и смыслу литературу в надежде предоставить читателям больше вариантов отыскать новые, интересные, ещё непрочитанные произведения.






Обсуждение, отзывы о книге «Managing Medical and Obstetric Emergencies and Trauma» и просто собственные мнения читателей. Оставьте ваши комментарии, напишите, что Вы думаете о произведении, его смысле или главных героях. Укажите что конкретно понравилось, а что нет, и почему Вы так считаете.