Veterinary Endoscopy for the Small Animal Practitioner
Здесь есть возможность читать онлайн «Veterinary Endoscopy for the Small Animal Practitioner» — ознакомительный отрывок электронной книги совершенно бесплатно, а после прочтения отрывка купить полную версию. В некоторых случаях можно слушать аудио, скачать через торрент в формате fb2 и присутствует краткое содержание. Жанр: unrecognised, на английском языке. Описание произведения, (предисловие) а так же отзывы посетителей доступны на портале библиотеки ЛибКат.
- Название:Veterinary Endoscopy for the Small Animal Practitioner
- Автор:
- Жанр:
- Год:неизвестен
- ISBN:нет данных
- Рейтинг книги:4 / 5. Голосов: 1
-
Избранное:Добавить в избранное
- Отзывы:
-
Ваша оценка:
Veterinary Endoscopy for the Small Animal Practitioner: краткое содержание, описание и аннотация
Предлагаем к чтению аннотацию, описание, краткое содержание или предисловие (зависит от того, что написал сам автор книги «Veterinary Endoscopy for the Small Animal Practitioner»). Если вы не нашли необходимую информацию о книге — напишите в комментариях, мы постараемся отыскать её.
Covers diagnostic endoscopy, interventional endoscopy, and minimally invasive soft tissue surgery Includes thousands of images to illustrate endoscopy concepts for veterinarians Provides a clinically oriented reference book for using rigid and flexible endoscopy in a small animal practice Supports veterinarians who are seeking to increase their services and enhance their revenue streams Any practitioner who is using or preparing to use endoscopic techniques will find
an essential practice resource.
Veterinary Endoscopy for the Small Animal Practitioner — читать онлайн ознакомительный отрывок
Ниже представлен текст книги, разбитый по страницам. Система сохранения места последней прочитанной страницы, позволяет с удобством читать онлайн бесплатно книгу «Veterinary Endoscopy for the Small Animal Practitioner», без необходимости каждый раз заново искать на чём Вы остановились. Поставьте закладку, и сможете в любой момент перейти на страницу, на которой закончили чтение.
Интервал:
Закладка:

Figure 1.7 An image through a coherent fiber bundle of a flexible fiberoptic gastroscope showing a subtle individual glass fiber pattern. This is a high‐quality image with small fibers and minimal inter fiber space producing little interference with the image.
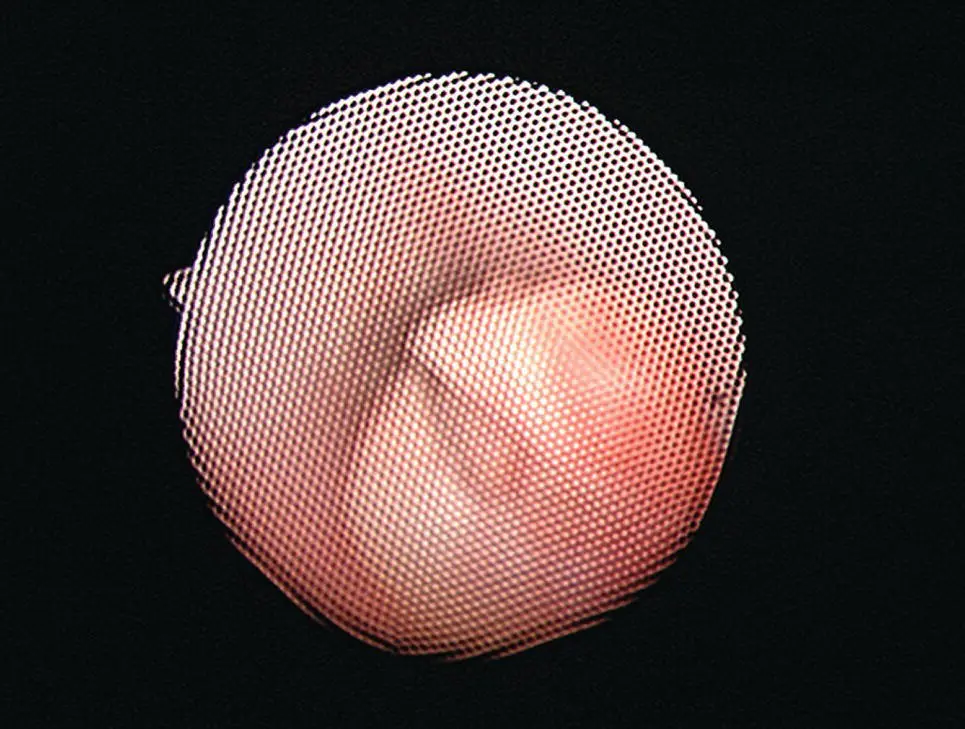
Figure 1.8 An image through a coherent fiber bundle of a flexible fiberoptic urethroscope showing a marked individual glass fiber pattern. This is an image of lesser quality due to the size of the fibers and thickness of the inter fiber space producing significant interference with the image.
The fibers of incoherent fiber bundles are randomly arranged and are used to transmit light from the light source into the patient and are called light guide cables or bundles. They do not transmit an image. The individual fibers in incoherent bundles are thicker than in image or coherent bundles making them more efficient at transmitting light. Flexible endoscopes will have one or two incoherent fiber bundles for the transmission of light from the light source to the distal tip. Rigid endoscopic telescopes use an incoherent flexible fiberoptic light guide cable to transmit light from the large external light source to the light post of the telescope. An incoherent fiber bundle is also present in the telescope to transmit light from the connection with the light guide cable at the light post to the tip of the telescope. This allows a bright powerful light to be transmitted to the end of the endoscope and into the body with a minimum of heat ( Figure 1.9).

Figure 1.9 The light transmission system for a rigid endoscopic telescope with the large external remote “cold light source” shown as a box, the flexible fiberoptic light cable seen as a coiled gray cord attached to the light source on one end, attached to the light guide post of a telescope at the other end, and there is a fiberoptic light guide bundle in the rigid telescope continuing from the light post through the telescope shaft to conduct light to the tip of endoscope. This light transmission system is composed of incoherent fiber bundles. The image of rigid telescopes is transmitted through a series of solid glass lenses.
( Source: Photo courtesy of Karl Storz: ©Karl Storz SE & Co KG, Germany.)
Another quantum leap forward critical to continuing the advance of endoscopy was the development of video camera systems specifically designed for endoscopy. Small lightweight camera heads ( Figure 1.10) made possible placing of the signal processing hardware in a separate remote box away from the endoscope. The camera head couples securely to either rigid telescopes ( Figure 1.11) or flexible endoscopes with a video image displayed on a monitor so that multiple people could see the endoscopic images simultaneously. This allowed all members of a surgical team to participate as assistants during procedures ( Figure 1.12). This technology made operative procedures possible and allowed the development of minimally invasive surgery. Initial cameras had a single CCD video chip, this was followed by three chip cameras, and then by high‐definition cameras. Another significant advance in endoscope technology was video endoscopes with a CCD chip at the tip of the endoscope ( Figure 1.13). This is most important in flexible endoscopes with elimination of the pixilated fiber pattern to greatly improve image quality ( Figure 1.14). For many years, CCD chip size limited the diameter of flexible video endoscope to sizes greater than 10 mm restricting their use to gastrointestinal‐sized equipment. This has been overcome and with CMOS technology, flexible video endoscopes as small as 3 mm are currently available.

Figure 1.10 A small lightweight endoscopy video camera head with a separate remote box containing the video signal processing hardware. A Karl Storz Endoscopy IMAGE I FULL HD camera control box on the bottom, an Image 1 capture module on the top, and a 3 chip HD camera head on top of the capture module.
( Source: Photo courtesy of Karl Storz: ©Karl Storz SE & Co KG, Germany.)
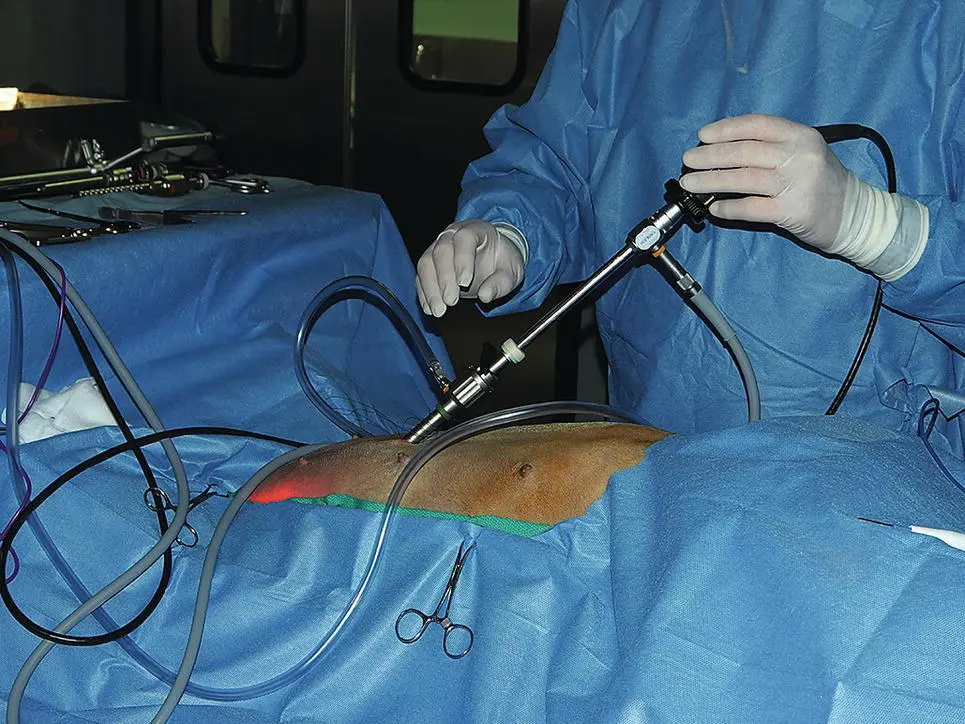
Figure 1.11 An endoscopy video camera head coupled to a 10 mm diameter laparoscope making a functionally one‐piece unit allowing easy examination and surgery with a stable video image of the telescope field of view.

Figure 1.12 A surgery team utilizing video for laparoscopic surgery where all members of the team can see the image on the video monitor.

Figure 1.13 A video gastroscope with a video camera chip at the tip of the endoscope with elimination of the image guide bundle and the eyepiece at the handle of the endoscope.
( Source: Photo courtesy of Karl Storz: ©Karl Storz SE & Co KG, Germany.)

Figure 1.14 An image of the duodenum in an 8‐year‐old neutered male 10 kg mixed breed dog with IBD illustrating the superior image produced with a video gastroscope.
Three‐dimensional video systems have been attempted for many years, but none have become popular or achieved a significant market presence. A recently released computer‐enhanced dual image system with significant improvement of image function may change this position for this technology.
Computer‐enhanced image technology has also entered the market with image manipulation to increase the visibility of normal and abnormal tissues. Photodynamic analysis systems are available that use fluorescing dyes combined with specific wavelength light sources, filters, and cameras facilitating the identification of tumors used to improve early diagnosis.
1.3 Clinical Application in Veterinary Medicine
Use of endoscopy in animals was listed in the early history of endoscopy in human medicine but it was not a clinical application and is not relevant to our history. At the time I graduated from Veterinary School in 1969, endoscopy was not a part of our clinical discussions. Endoscopy in small animal veterinary medicine first appeared in the early 1970s. Endoscopic evaluation of the lower respiratory tract in dogs and cats was first reported in 1970 (O'Brien 1970). The first use of laparoscopy for the evaluation of liver and pancreatic disease was reported in 1972 (Dalton and Hill 1972; Lettow 1972). The first reported use of gastrointestinal endoscopy in practice was in 1976 (Johnson et al. 1976). Gastrointestinal endoscopy developed widespread clinical application before any other techniques and has been the most frequently used endoscopic procedure in small animal medicine. Bronchoscopy also gained wide acceptance during this time period.
Читать дальшеИнтервал:
Закладка:
Похожие книги на «Veterinary Endoscopy for the Small Animal Practitioner»
Представляем Вашему вниманию похожие книги на «Veterinary Endoscopy for the Small Animal Practitioner» списком для выбора. Мы отобрали схожую по названию и смыслу литературу в надежде предоставить читателям больше вариантов отыскать новые, интересные, ещё непрочитанные произведения.









Обсуждение, отзывы о книге «Veterinary Endoscopy for the Small Animal Practitioner» и просто собственные мнения читателей. Оставьте ваши комментарии, напишите, что Вы думаете о произведении, его смысле или главных героях. Укажите что конкретно понравилось, а что нет, и почему Вы так считаете.