Kelly Vana's Nursing Leadership and Management
Здесь есть возможность читать онлайн «Kelly Vana's Nursing Leadership and Management» — ознакомительный отрывок электронной книги совершенно бесплатно, а после прочтения отрывка купить полную версию. В некоторых случаях можно слушать аудио, скачать через торрент в формате fb2 и присутствует краткое содержание. Жанр: unrecognised, на английском языке. Описание произведения, (предисловие) а так же отзывы посетителей доступны на портале библиотеки ЛибКат.
- Название:Kelly Vana's Nursing Leadership and Management
- Автор:
- Жанр:
- Год:неизвестен
- ISBN:нет данных
- Рейтинг книги:5 / 5. Голосов: 1
-
Избранное:Добавить в избранное
- Отзывы:
-
Ваша оценка:
Kelly Vana's Nursing Leadership and Management: краткое содержание, описание и аннотация
Предлагаем к чтению аннотацию, описание, краткое содержание или предисловие (зависит от того, что написал сам автор книги «Kelly Vana's Nursing Leadership and Management»). Если вы не нашли необходимую информацию о книге — напишите в комментариях, мы постараемся отыскать её.
Includes new and up-to-date information from national and state health care and nursing organizations, as well as new chapters on the historical context of nursing leadership and management and the organization of patient care in high reliability health care organizations Explores each of the six Quality and Safety in Nursing (QSEN) competencies: Patient-Centered Care, Teamwork and Collaboration, Evidence-based Practice (EBP), Quality Improvement (QI), Safety, and Informatics Provides review questions for all chapters to help students prepare for course exams and NCLEX state board exams Features contributions from experts in the field, with perspectives from bedside nurses, faculty, directors of nursing, nursing historians, physicians, lawyers, psychologists and more
provides a strong foundation for evidence-based, high-quality health care for undergraduate nursing students, working nurses, managers, educators, and clinical specialists.
Kelly Vana's Nursing Leadership and Management — читать онлайн ознакомительный отрывок
Ниже представлен текст книги, разбитый по страницам. Система сохранения места последней прочитанной страницы, позволяет с удобством читать онлайн бесплатно книгу «Kelly Vana's Nursing Leadership and Management», без необходимости каждый раз заново искать на чём Вы остановились. Поставьте закладку, и сможете в любой момент перейти на страницу, на которой закончили чтение.
Интервал:
Закладка:
Comprehensiveness: Manage the wide range of health care needs, across health care settings and among different health care professionals.
Coordination: Build upon longitudinality. Care received through referrals and other providers is followed and integrated, averting unnecessary services and duplication of services.
Case Study 2.1
You work in an Emergency Department (ED) that sees 6,000 patients a month. Patients are charged at least $200.00 per visit plus charges for tests and medications. Thus, these 6,000 patients can generate $1,200,000 in gross revenue for the hospital. Consider that there are 15 RNs making $30.00 hr and 6 MDs, making $150.00 hr working each shift. Salaries for the RNs total $324,000. Salaries for the MDs total $648,000. The total salary for these two groups is $972,000. Of the 6,000 patients, 50% have Medicare/Medicaid, 45% are covered by managed care or insurance, and 5% have no insurance. Thus, just 95% of patients can pay their bills. The other 5% of patient's bills are written off by the hospital as bad debt.
Medicare/Medicaid/Managed Care/Insurance companies often pay only 55% of the bills for these patients. They may deny payment for 45% of the bills. Thus, for the $1,140,000 billed (95% of $1,200,000), the hospital will receive approximately $627,000 (55% of the $1,140,000 billed). Approximately $513,000 of the bill will not be paid by Medicare/Medicaid/Managed Care/Insurance. Consider the following:
What other expenses besides salary must the hospital pay out of the $627,000 that it receives? Consider hospital space, liability insurance, technology costs, and so on.
Notice the effect that increasing the volume of patients has on your budget figures. What happens to your budget if the patient volume goes to 8,000 patient ED visits per month and staffing stays the same?
Are patients receiving useful information about future illness prevention and healthy living practices in the ED?
Is this a cost‐effective way to deliver health care?
How could we better serve the health care needs of Americans?
Primary care clinicians, which primarily include both medical and nursing practitioners, can be a patient's greatest asset in negotiating the health care system and improving patient outcomes. It is through understanding the patient's past and present that future health care needs can be anticipated. Primary care interventions, such as health promotion and timely preventive care and medication administration, can reduce the need for hospitalizations, improve the health of patients, and avert adverse morbidity and mortality outcomes. Patients and their families can communicate with clinicians to understand their health care needs, how to achieve the best possible health, and how to partner with clinicians to improve decision making. This is what patient‐centered care is based on, both primary care and patient decision making. The World Health Report (2008b), Primary Health Care: Now More than Ever , underscores the need for primary health care. The report cites a disproportionate focus on specialist hospital care, fragmentation of health systems, and the proliferation of unregulated commercial care. The WHO (2010b) has also identified key elements in improving health status through primary care strategies aimed at reducing disparities through universal access, enhancing coordination and delivery of care, and increasing stakeholder participation at multiple levels.
The Federal Government
The federal government is a major driver of health care organization and delivery. Distinct, major divisions of the U.S. Department of Health and Human Services(DHHS) include the following:
Agency for Healthcare Research and Quality (AHRQ): Funds health services research on the effectiveness of health care services and outcomes of care.
Centers for Disease Control and Prevention (CDC): Promotes health and quality of life by preventing and controlling disease, injury, and disability.
Centers for Medicare and Medicaid Services (CMS): Administers the Medicare program and regulates the Medicaid program.
Food and Drug Administration (FDA): Monitors the safety of food, the safety of cosmetic products, the safety and efficacy of drugs, and the safety and efficacy of medical devices.
Health Resources and Services Administration (HRSA): Administers training programs for health care clinicians, funding for pregnant women and children, programs for persons with HIV/AIDS, and programs serving low‐income, underserved, and rural populations.
Indian Health Service (IHS): Maintains health services provided to American Indians and Alaska Natives (ANs).
National Institutes of Health (NIH): Funds biomedical research through 18 research institutes primarily organized according to specific diseases.
Substance Abuse and Mental Health Services Administration (SAMHSA): Provides leadership in services, policy, and information dissemination for mental health and substance abuse treatment and prevention.
State and Local Levels
Public health services at the state and local levels include boards of health and state and local health departments. Even with the 1988 IOM Report on public health, the ability of public health departments to engage in improving the health of the public has become limited (Tilson & Berkowitz, 2006). In addition, efforts for bioterrorism and disaster preparedness have brought the nation's infrastructure desolation to light, causing increased funding for this nation's disaster preparedness efforts, with little money focused on public health care funding and infrastructure redevelopment.
Home Health Care
The location of care delivery is continually changing to adapt to technologies and patient needs. The use of home health care services continues to grow as more and more individuals access these services in the community setting, in lieu of institutional care. According to the Centers for Medicare and Medicaid Services (CMS) (2018), home health care expenditures were 3% of national health care expenditures in 2017, of the overall spending of having reached $3.5 trillion. This increase has been primarily driven by higher growth in Medicaid spending, partly due to Medicaid's continued shifting of long‐term care from institutional to home settings. In light of an aging population, home health care services will continue to serve an integral role in health care delivery.
Health Care Disparities and Social Determinants of Health
Inequalities in such things as gender, age, ethnicity, etc. ( Figure 2.3) have been recognized as great influences on health outcomes. Socioeconomic status is the number one predictor of poor health. The 2018 NHDR found from 2000 to 2017 (AHRQ, 2019):
More than half of access measures showed improvement.
One‐third of access measures did not show improvement.
Fourteen percent showed worsening.
Blacks, American Indians and Alaska Natives (AI/ANs), and Native Hawaiians/Pacific Islanders (NHPIs) received worse care than Whites for about 40% of quality measures.
Hispanics received worse care than Whites for about 35% of quality measures.
Asians received worse care than Whites for 27% of quality measures, but better care than Whites for 28% of quality measures
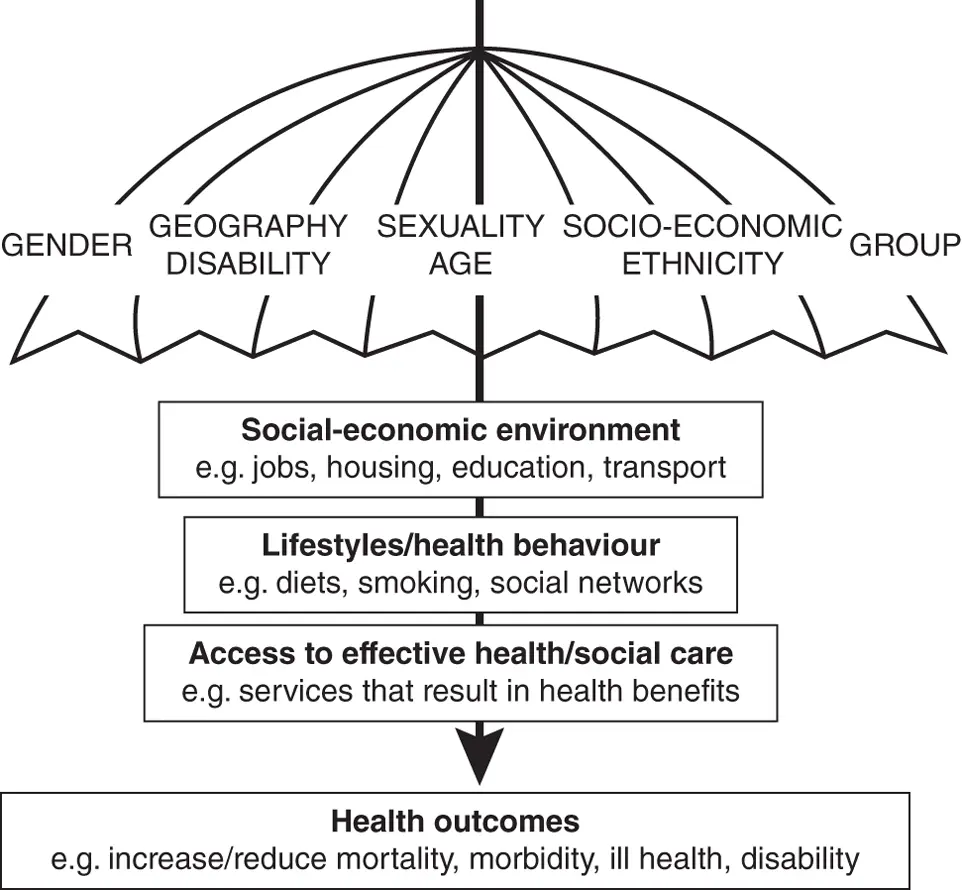 FIGURE 2.3 The spectrum of inequality.
FIGURE 2.3 The spectrum of inequality.
Source: https://www.nationalarchives.gov.uk/doc/open‐government‐licence/version/3/ Contains Parliamentary information licensed under the Open Parliament Licence v3.0
The report also noted, even when the overall quality of care improves, health care disparities often still persist across socioeconomic groups, racial and ethnic populations, and geographical areas (AHRQ, 2019). In addition, not enough health care delivery and attention is directed toward the top underlying causes of death in the United States ( Table 2.2).
Читать дальшеИнтервал:
Закладка:
Похожие книги на «Kelly Vana's Nursing Leadership and Management»
Представляем Вашему вниманию похожие книги на «Kelly Vana's Nursing Leadership and Management» списком для выбора. Мы отобрали схожую по названию и смыслу литературу в надежде предоставить читателям больше вариантов отыскать новые, интересные, ещё непрочитанные произведения.







Обсуждение, отзывы о книге «Kelly Vana's Nursing Leadership and Management» и просто собственные мнения читателей. Оставьте ваши комментарии, напишите, что Вы думаете о произведении, его смысле или главных героях. Укажите что конкретно понравилось, а что нет, и почему Вы так считаете.