Fernando Suarez - Periodontics
Здесь есть возможность читать онлайн «Fernando Suarez - Periodontics» — ознакомительный отрывок электронной книги совершенно бесплатно, а после прочтения отрывка купить полную версию. В некоторых случаях можно слушать аудио, скачать через торрент в формате fb2 и присутствует краткое содержание. Жанр: unrecognised, на английском языке. Описание произведения, (предисловие) а так же отзывы посетителей доступны на портале библиотеки ЛибКат.
- Название:Periodontics
- Автор:
- Жанр:
- Год:неизвестен
- ISBN:нет данных
- Рейтинг книги:5 / 5. Голосов: 1
-
Избранное:Добавить в избранное
- Отзывы:
-
Ваша оценка:
Periodontics: краткое содержание, описание и аннотация
Предлагаем к чтению аннотацию, описание, краткое содержание или предисловие (зависит от того, что написал сам автор книги «Periodontics»). Если вы не нашли необходимую информацию о книге — напишите в комментариях, мы постараемся отыскать её.
Periodontics — читать онлайн ознакомительный отрывок
Ниже представлен текст книги, разбитый по страницам. Система сохранения места последней прочитанной страницы, позволяет с удобством читать онлайн бесплатно книгу «Periodontics», без необходимости каждый раз заново искать на чём Вы остановились. Поставьте закладку, и сможете в любой момент перейти на страницу, на которой закончили чтение.
Интервал:
Закладка:
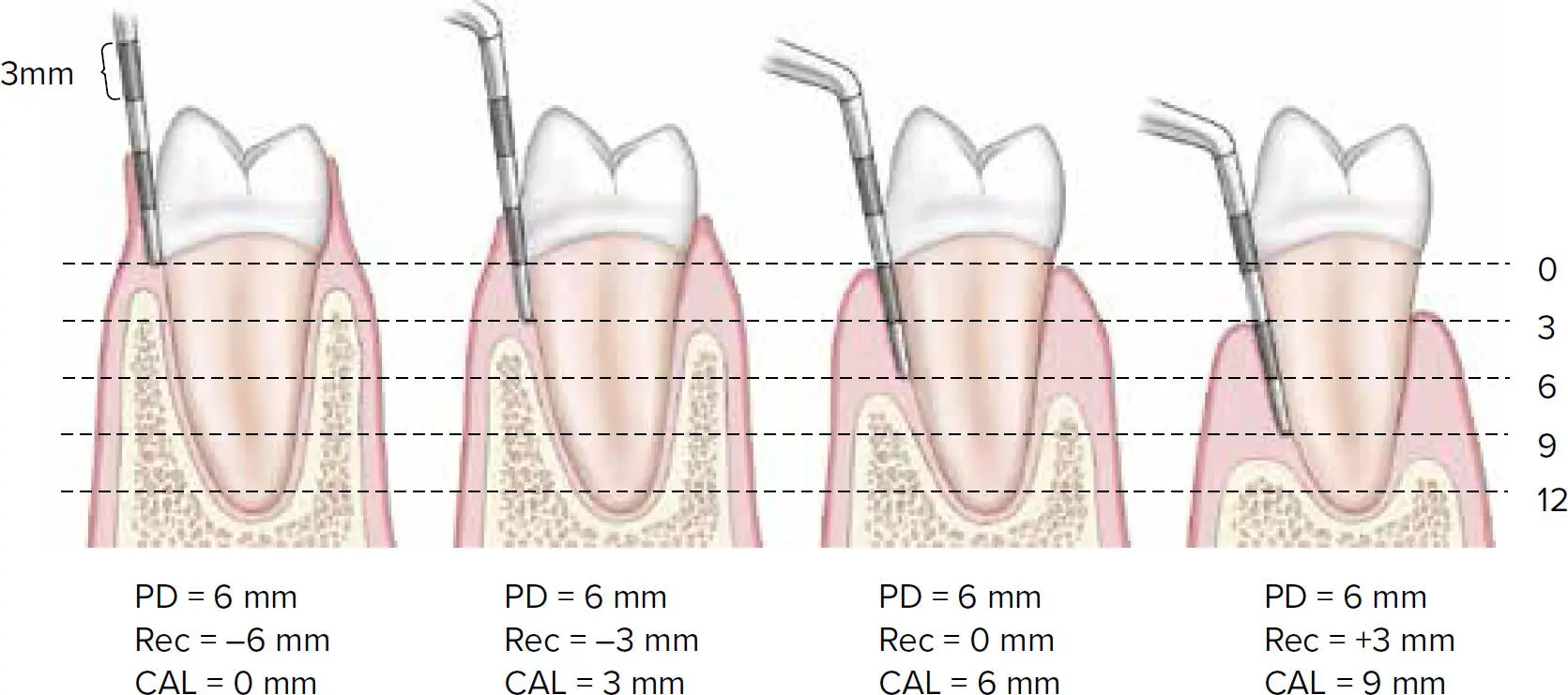
Fig 2-1 Representation of different situations with 6 mm PD and different attachment levels. Rec, recession.
ATTACHED GINGIVA AND KERATINIZED GINGIVA
The amount of AG and the width of KG are also important clinical parameters to record during a comprehensive periodontal evaluation. AG extends from the free gingival marginal groove to the mucogingival junction (MGJ), and it is the portion of the gingiva bonded to the tooth and the alveolar bone through gingival fibers 1(Fig 2-2). On the other hand, KG includes free (marginal) gingiva and the AG. Around teeth, healthy and uninflamed gingival tissue usually encompass a band of AG, which is crucial to defend against pathogens. 2
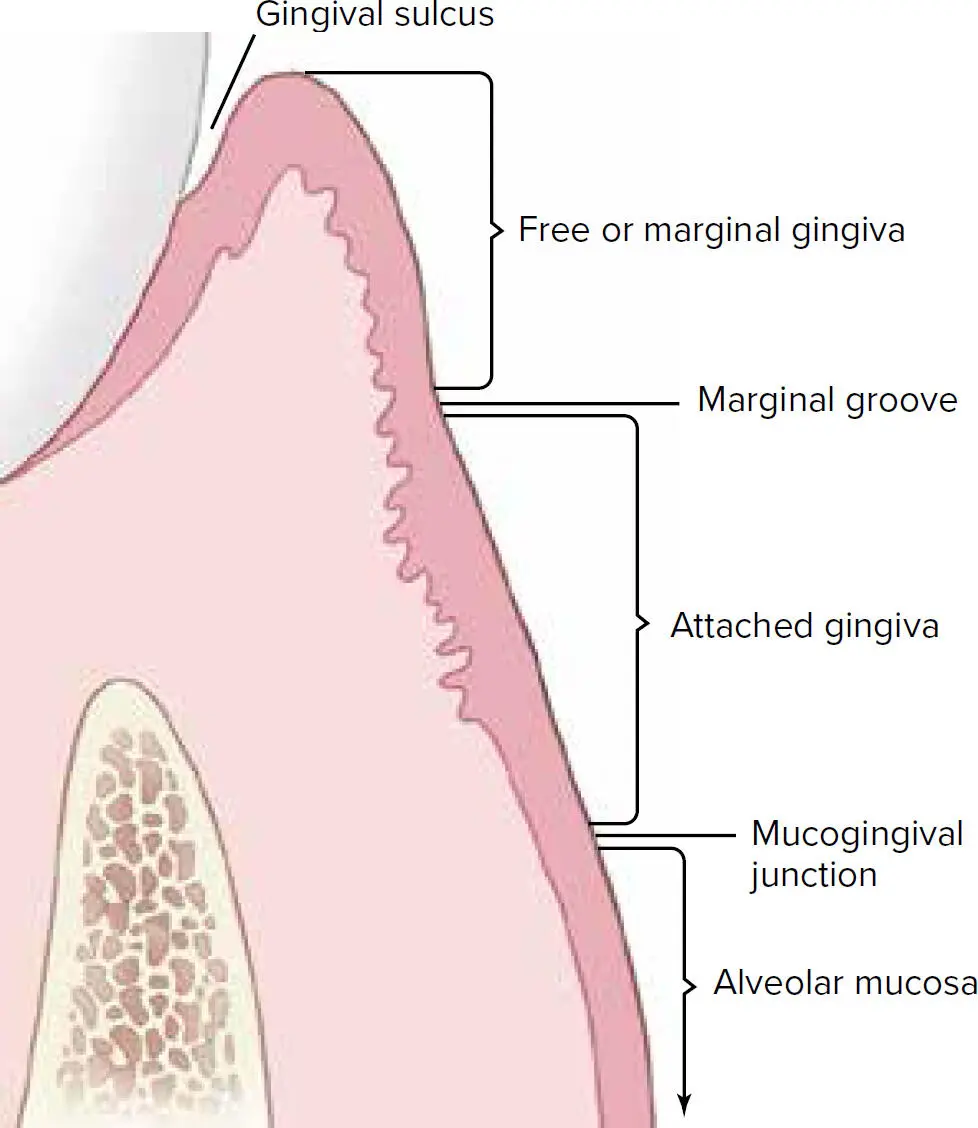
Fig 2-2 Gingival landmarks.
Lang and Löe performed a clinical study evaluating the inflammation status by examining gingival exudate of teeth with or without 2 mm of KG. 16The results from this investigation indicated that most teeth with < 2 mm of KG presented with clinical inflammation and varying amounts of exudate while surfaces with ≥ 2 mm of KG were healthy, and most of these surfaces showed no exudate. 16Therefore, it was concluded that 2 mm of KG and 1 mm of AG are needed to maintain periodontal stability. 16Nevertheless, evidence from another study demonstrated that when good plaque control is achieved through adequate home care, the presence of AG/KG is not an essential prerequisite for the maintenance of periodontal health and attachment. 17Overall, it is generally accepted that the presence of a collar of KG and AG is beneficial for the long-term stability of the periodontium, and even more important when oral hygiene is not optimal. The MGJ and the width of KG can be determined using the methods demonstrated in Fig 2-3 and Box 2-2. 2,16

Fig 2-3 Visual examination of the MGJ. The arrow indicates the junction between the KG and the mucosa. KG presents as a coral pink color, while mucosa is redder.
BOX 2-2 Methods to determine the location of MGJ and the width of KG 3,16
| VisualExamine for color difference. AG/KG of healthy gingiva usually presents a coral pink coloration, while mucosa is darker and redder (see Fig 2-3). Schiller’s iodine testOral mucosa can be stained with an iodine solution because of the glycogen distribution, while KG is iodine-negative. 16 Roll techniqueOral mucosa is movable while AG/KG is bonded to tooth surface and bone. A clear demarcation (MGJ) would appear when rolling from movable mucosa to AG/KG. |
BLEEDING ON PROBING
BOP is another important parameter to record during periodontal examination, and it indicates evidence of gingival inflammation. A prospective study by Lang and colleagues evaluated the prognostic value of sites with BOP and the risk for periodontal breakdown of at least 2 mm of attachment loss during periodontal maintenance therapy. 18The results showed that only a 30% probability of future attachment loss may be predicted for sites repeatedly positive for BOP ( Table 2-2). 18Further calculations confirmed that frequent BOP for prediction of future attachment loss yields a specificity of 88%, and the continuous absence of BOP has a positive predictive value of 98%. 19Therefore, it is of paramount importance to understand that BOP alone does not represent a good positive predictor for disease progression 7; instead, studies have shown that absence of BOP is a more reliable parameter to indicate periodontal stability. 19BOP is also sensitive to the forces applied with the probe 2,19; therefore, Lang et al suggested a probing force of 25 g (0.25 N) when recording BOP, as heavier pressures (> 25 g) might traumatize the gingival tissue and provoke bleeding. 19In conclusion, the presence of BOP has low sensitivity and high specificity with respect to the development of additional attachment loss. For clinicians to monitor patients’ periodontal stability over time in daily practice, the absence of BOP at 25 g is a reliable indicator for periodontal stability with a negative predictive value of 98%. 7,18,19
TABLE 2-2 Positive predictive values for loss of attachment of ≥ 2 mm in 2 years in sites that bled on probing 0, 1, 2, 3, or 4 times out of 4 maintenance visits 18
| BOP incidence | Sites with loss of attachment > 2 mm |
| 4/4 | 30% |
| 3/4 | 14% |
| 2/4 | 6% |
| 1/4 | 3% |
| 0/4 | 1.5% |
FURCATION INVOLVEMENT
The furcation is the anatomical area of a multirooted tooth from where the roots diverge and form bifurcation (two-rooted tooth) or trifurcation (three-rooted tooth). 2 Furcation involvement or furcation invasion describes the pathologic resorption of bone within a furcation area 1,2,20(Fig 2-4). The Nabers furcation probe is widely used and suited for detection and examination of furcation involvement. 2,20The extent and configuration of furcation involvement can be characterized by anatomical factors including but not limited to presence of cervical enamel projections, enamel pearls, root trunk distance, tooth surface concavities, and the extent of root separation. The following summarizes the furcation entrances of multirooted teeth to aid in detection of furcation involvement 20:

Fig 2-4 Furcation entrance on a mandibular first molar.
Maxillary premolar:Furcation involvement can be detected from the mesial or distal surface; the entrance is located at the apical third of the root and/or approximately 8 mm below the CEJ.
Maxillary molars:Buccal entrance: Centered mesiodistally.Mesial entrance: Two-thirds of the buccolingual width toward the palatal aspect, easier to approach from mesiopalatal aspect.Distal entrance: Furcation entrance is centered buccolingually and can be examined from either the buccal or palatal aspect.
Mandibular molars:Buccal entrance: Centered mesiodistally at the buccal surface.Lingual entrance: Centered mesiodistally at the lingual surface.
The amount of furcation involvement of a multirooted tooth can be registered depending on the horizontal and vertical amount of bony destruction into the furcation area. 20–22Many systems have been proposed for classifying furcation involvement. 2Hamp’s classification is one of the most commonly used for furcation destruction. 22A brief review of three systems is presented in the following sections. 2,20–23
Horizontal destruction
Glickman (1958) divided furcation involvement into 4 grades 21:
Grade I: Pocket formation into the flute but intact interradicular bone. Incipient lesion.
Grade II: Loss of interradicular bone and pocket formation of varying depths into the furcation area but not completely through to the opposite side of the tooth.
Grade III: Through-and-through lesion.
Grade IV: Same as Grade III with through-and-through lesion with gingival recession, rendering the furcation area clearly visible on clinical examination.
Читать дальшеИнтервал:
Закладка:
Похожие книги на «Periodontics»
Представляем Вашему вниманию похожие книги на «Periodontics» списком для выбора. Мы отобрали схожую по названию и смыслу литературу в надежде предоставить читателям больше вариантов отыскать новые, интересные, ещё непрочитанные произведения.




Обсуждение, отзывы о книге «Periodontics» и просто собственные мнения читателей. Оставьте ваши комментарии, напишите, что Вы думаете о произведении, его смысле или главных героях. Укажите что конкретно понравилось, а что нет, и почему Вы так считаете.