Fernando Suarez - Periodontics
Здесь есть возможность читать онлайн «Fernando Suarez - Periodontics» — ознакомительный отрывок электронной книги совершенно бесплатно, а после прочтения отрывка купить полную версию. В некоторых случаях можно слушать аудио, скачать через торрент в формате fb2 и присутствует краткое содержание. Жанр: unrecognised, на английском языке. Описание произведения, (предисловие) а так же отзывы посетителей доступны на портале библиотеки ЛибКат.
- Название:Periodontics
- Автор:
- Жанр:
- Год:неизвестен
- ISBN:нет данных
- Рейтинг книги:5 / 5. Голосов: 1
-
Избранное:Добавить в избранное
- Отзывы:
-
Ваша оценка:
Periodontics: краткое содержание, описание и аннотация
Предлагаем к чтению аннотацию, описание, краткое содержание или предисловие (зависит от того, что написал сам автор книги «Periodontics»). Если вы не нашли необходимую информацию о книге — напишите в комментариях, мы постараемся отыскать её.
Periodontics — читать онлайн ознакомительный отрывок
Ниже представлен текст книги, разбитый по страницам. Система сохранения места последней прочитанной страницы, позволяет с удобством читать онлайн бесплатно книгу «Periodontics», без необходимости каждый раз заново искать на чём Вы остановились. Поставьте закладку, и сможете в любой момент перейти на страницу, на которой закончили чтение.
Интервал:
Закладка:
Hamp et al (1975) proposed three levels of furcation involvement 22(Fig 2-5):
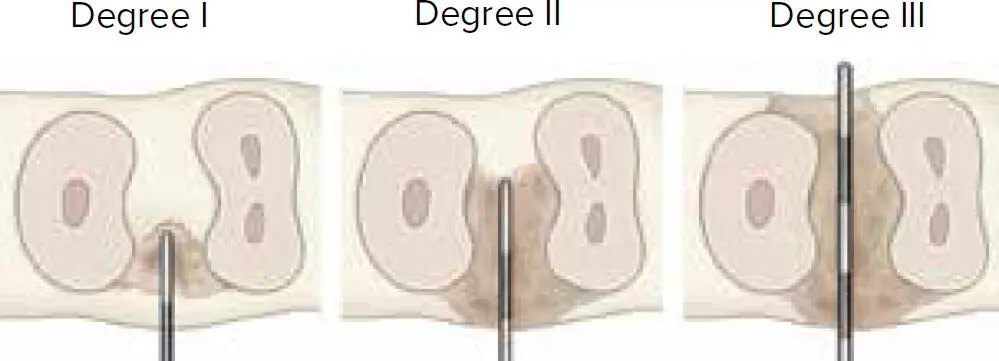
Fig 2-5 Different degrees of furcation involvement.
Degree I: Horizontal loss of periodontal tissue support < 3 mm.
Degree II: Horizontal loss > 3 mm, but not passing the total width of the furcation.
Degree III: Horizontal through-and-through destruction.
Vertical destruction
Tarnow and Fletcher (1985) proposed the following classification based on the vertical bone loss around furcations. It is encouraged to supplement each category of horizontal destruction with a subclass based on the vertical bone resorption. 23
Subclass A: 0 to 3 mm probeable depth.
Subclass B: 4 to 6 mm probeable depth.
Subclass C: ≥ 7 mm probeable depth.
MOBILITY
The definition of tooth mobility is the movement of a tooth in its socket resulting from an applied force. 1Increase in tooth mobility is often a sign of periodontal breakdown and/or presence of excessive occlusal forces. 1Tooth mobility is detected by using the ends of two instruments (eg, mirror handle) on either side of the tooth and alternately applying forces. 2The most commonly used clinical index for tooth mobility is the Miller Index; using this index, mobility can be scored as the following 2,24:
Class 0: Normal (physiologic) movement when force is applied. It has been defined as movement up to 0.2 mm horizontally and 0.02 mm axially.
Class I: First distinguishable sign of movement greater than “normal” or “physiologic.”
Class II: Movement of the crown up to 1 mm in any direction (buccolingual or mesiodistal).
Class III: Movement of the crown more than 1 mm in any direction (buccolingual or mesiodistal) and/or vertical depression (apicocoronal) or rotation of the crown in its socket.
Radiographic Interpretation
Clinical periodontal examination provides information with regard to PDs, recession defects, AG/KG, and more; however, it cannot reveal the status of the alveolar bone. The alveolar bone is another critical aspect to take into consideration to accurately diagnose different periodontal diseases and conditions. 2Dental radiographs are the most commonly used noninvasive method of examining alveolar bone levels. Other valuable information that can be obtained through radiographic examination includes subgingival calculus deposition, root length and form, crown-to-root ratio, presence of periapical lesions, periodontal ligament space, root proximity, and the destruction of alveolar bone. 2,7
Clinicians should keep in mind the following limitations of conventional dental radiography when interpreting radiographs during the examination phase 3,7,25:
Radiographs do not show periodontal pockets. 25
Radiographs cannot distinguish between posttreatment periodontitis and active periodontitis. 25
Radiographs do not show buccal and lingual aspects of tooth and alveolar bone. 25
Radiographs cannot detect tooth mobility. 25
Radiographs can provide evidence of past destruction to the periodontium, but they cannot identify sites with active or ongoing periodontal inflammation. 7
Clinical attachment loss always precedes visual radiographic changes by approximately 6 to 8 months, and clinical attachment variations are greater than radiographic changes. 26
Radiographic changes are detectable by simple visual inspection when approximately 30% to 50% of the bone mineral has been lost. 27
The presence or absence of the crestal lamina dura is another common interpretation of radiographs for diagnosing periodontitis. Rams et al 28observed that the presence of intact crestal lamina dura is positively correlated to periodontal stability over a 2-year follow up period. However, no significant relationship could be found between future periodontal breakdown and lack of crestal lamina dura. 28A recent publication by Rams et al also reported similar findings and concluded that patients with angular bony morphology and PD greater than 5 mm poses a significant risk of periodontitis progression after treatment. However, if intact crestal lamina dura is present, despite the bony morphology, clinical stability for at least 24 months can be anticipated. 29Also, molar furcation involvement can sometimes be observed on radiographs. Hardekopf et al were the first to describe the radiographic features of maxillary molars with furcation destruction: a triangular radiographic shadow, commonly known as “furcation arrow,” can be noted over the mesial and distal proximal areas of maxillary molars. 30The clinical reliability of the presence of furcation arrow can be subjective and also greatly dependent on the degree of destruction. For instance, when furcation arrows are present on radiographs, these can only predict actual furcation invasion 70% of the time. On the other hand, when there is true furcation involvement, a furcation arrow is seen in less than 40% of the sites. 31It has been reported that the presence of furcation arrow for diagnosing furcation involvement on maxillary molars has a low sensitivity (38.7%) and high specificity (92.2%). 31When mandibular molars suffer from furcation involvement, radiolucency can be noted at the area where roots start to separate.
In recent years, the utilization of CBCT has been rapidly increasing in popularity. CBCT has become an integral tool for researchers and clinicians, mostly applied to the implant field. As such, the use of CBCT imaging for the diagnosis of periodontitis has also been studied. However, in 2017, the American Academy of Periodontology reported that even though its use may be beneficial in selective cases, there is limited evidence to support the use of CBCT for the different types of bony defects, and there are no guidelines for its application to periodontal treatment planning. 32
Advanced and Emerging Examination
Periodontitis is a multifactorial disease involving the combination of dysbiosis of oral bacteria and an overreacted immune response from the host. 33One of the disadvantages of the clinical periodontal evaluation is that these examinations only record destruction that has already occurred, such as the bone loss pattern and periodontal pockets. Therefore, patients would greatly benefit from techniques that detect the development of periodontal inflammation before tissue breakdown occurs and prevent further complications such as bone loss, tooth mobility, and ultimately tooth loss. The major rationale to develop advanced methods for examination is to detect disease activity at a subclinical level in order to provide early diagnosis and create a treatment plan tailored to each individual. 34
Researchers and scientists have been investigating possible periodontitis-related biomarkers that could be used to distinguish between healthy and diseased patients. 34These biomarkers can be collected from saliva, which can demonstrate overall periodontal health at a subject level, or gingival crevicular fluid, which is site specific. 34For instance, proportions of specific periodontal pathogens, pro- and anti-inflammatory cytokines, and tissue-degradation products have all been studied to differentiate between healthy and periodontitis subjects. Among all biomarkers, interleukin-1 (IL-1) is one of the most notable proinflammatory cytokines that has been extensively studied in the periodontal field. 34,35Periodontal pathogens that have been extensively studied and proved to be closely linked to the development of periodontitis include Porphyromonas gingivalis , Treponema denticola , Tannerella forsythia , Aggregatibacter actinomycetemcomitans , Fusobacterium nucleatum , and more. 2,36Research in the field of advanced examination and biomarkers is still ongoing, and the results have indicated a promising future for early detection of periodontitis. However, these examinations are still not routinely utilized, due at least in part to the additional costs and disassociation to treatment options (ie, the test results would not alter the treatment plan). 34
Читать дальшеИнтервал:
Закладка:
Похожие книги на «Periodontics»
Представляем Вашему вниманию похожие книги на «Periodontics» списком для выбора. Мы отобрали схожую по названию и смыслу литературу в надежде предоставить читателям больше вариантов отыскать новые, интересные, ещё непрочитанные произведения.




Обсуждение, отзывы о книге «Periodontics» и просто собственные мнения читателей. Оставьте ваши комментарии, напишите, что Вы думаете о произведении, его смысле или главных героях. Укажите что конкретно понравилось, а что нет, и почему Вы так считаете.