Barbara J. Bain - Haematology
Здесь есть возможность читать онлайн «Barbara J. Bain - Haematology» — ознакомительный отрывок электронной книги совершенно бесплатно, а после прочтения отрывка купить полную версию. В некоторых случаях можно слушать аудио, скачать через торрент в формате fb2 и присутствует краткое содержание. Жанр: unrecognised, на английском языке. Описание произведения, (предисловие) а так же отзывы посетителей доступны на портале библиотеки ЛибКат.
- Название:Haematology
- Автор:
- Жанр:
- Год:неизвестен
- ISBN:нет данных
- Рейтинг книги:5 / 5. Голосов: 1
-
Избранное:Добавить в избранное
- Отзывы:
-
Ваша оценка:
Haematology: краткое содержание, описание и аннотация
Предлагаем к чтению аннотацию, описание, краткое содержание или предисловие (зависит от того, что написал сам автор книги «Haematology»). Если вы не нашли необходимую информацию о книге — напишите в комментариях, мы постараемся отыскать её.
Haematology: From the Image to the Diagnosis Haematology: From the Image to the Diagnosis
Haematology — читать онлайн ознакомительный отрывок
Ниже представлен текст книги, разбитый по страницам. Система сохранения места последней прочитанной страницы, позволяет с удобством читать онлайн бесплатно книгу «Haematology», без необходимости каждый раз заново искать на чём Вы остановились. Поставьте закладку, и сможете в любой момент перейти на страницу, на которой закончили чтение.
Интервал:
Закладка:
MCQ
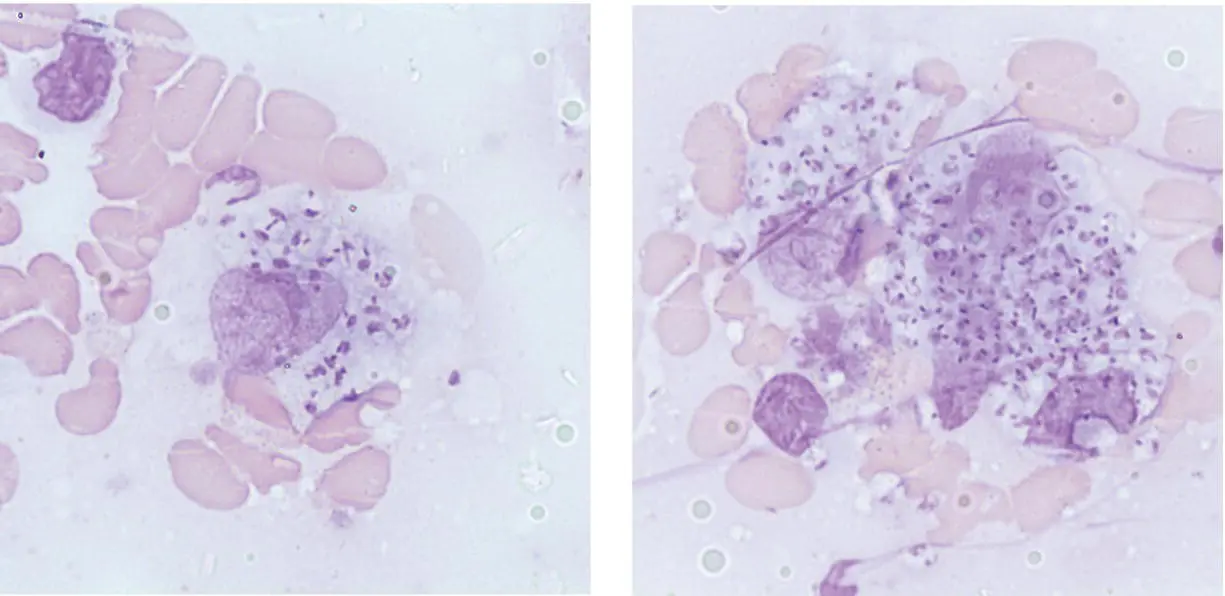
1 Leishmaniasis involving the bone marrow:Can be complicated by a haemophagocytic syndromeCan cause granuloma formationCan lead to significant dyserythropoiesisIs easily detected with Grocott’s methenamine silver stainIs often associated with increased plasma cellsFor answers and discussion, see page 206.
8 Gelatinous transformation of the bone marrow
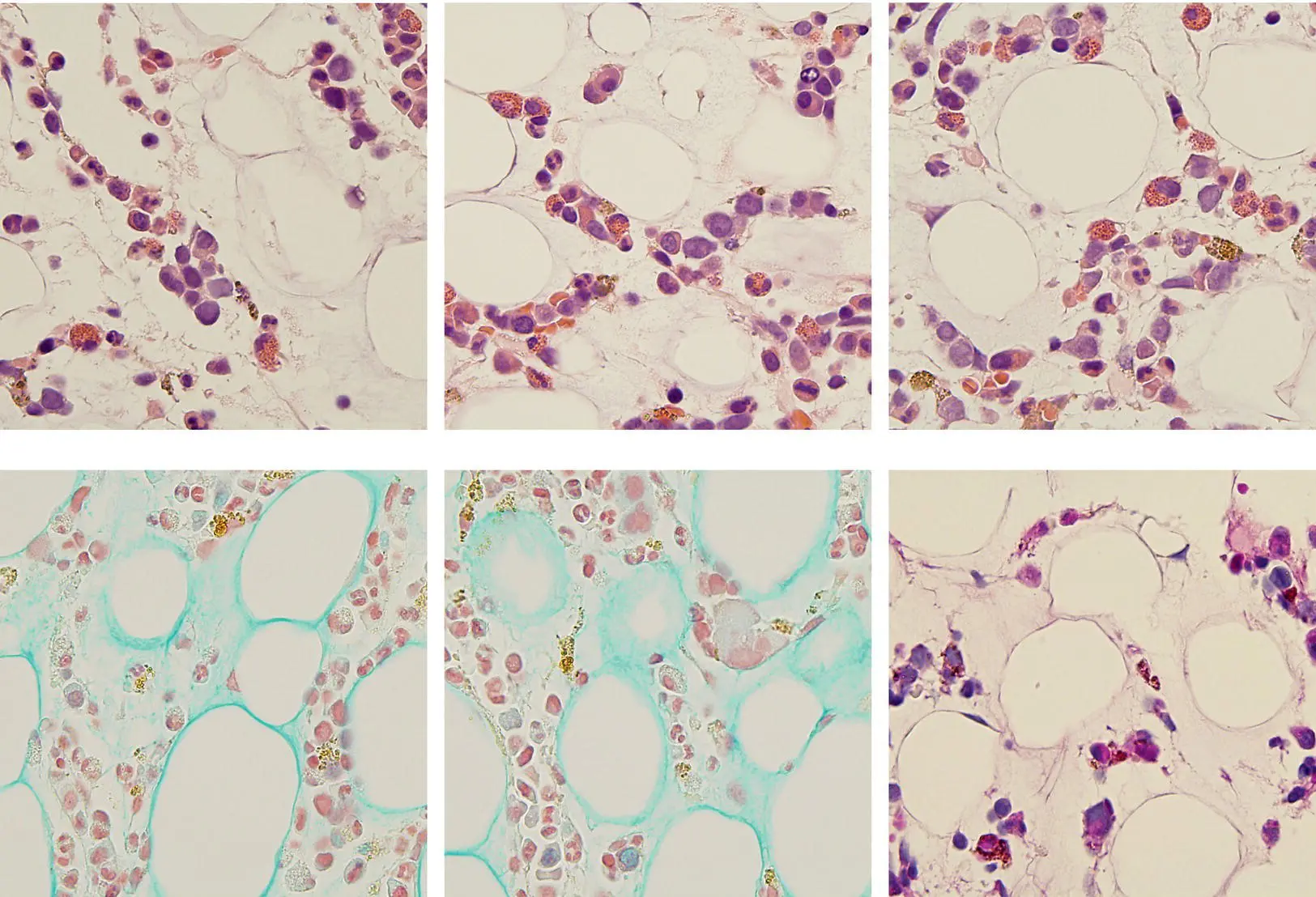
A 60‐year‐old man with chronic debility due to neurosarcoidosis was referred for investigation of a normocytic anaemia with Hb 100 g/l and normal leucocyte and platelet counts. The blood film was not informative. He underwent bone marrow aspiration. The aspirate was hypocellular but did not show any definitive diagnostic features. The bone marrow trephine biopsy specimen was abnormal, showing hypocellularity with reduction of haemopoietic activity around the marrow fat spaces (top images, H&E) (all images ×50 objective). The hypocellular areas show preserved architecture and an amorphous myxoid (mucoid) interstitium. Subsequent staining with Alcian blue (bottom left and centre) and periodic acid–Schiff (bottom right) confirmed the diagnosis of gelatinous transformation, also known as myxoid degeneration.
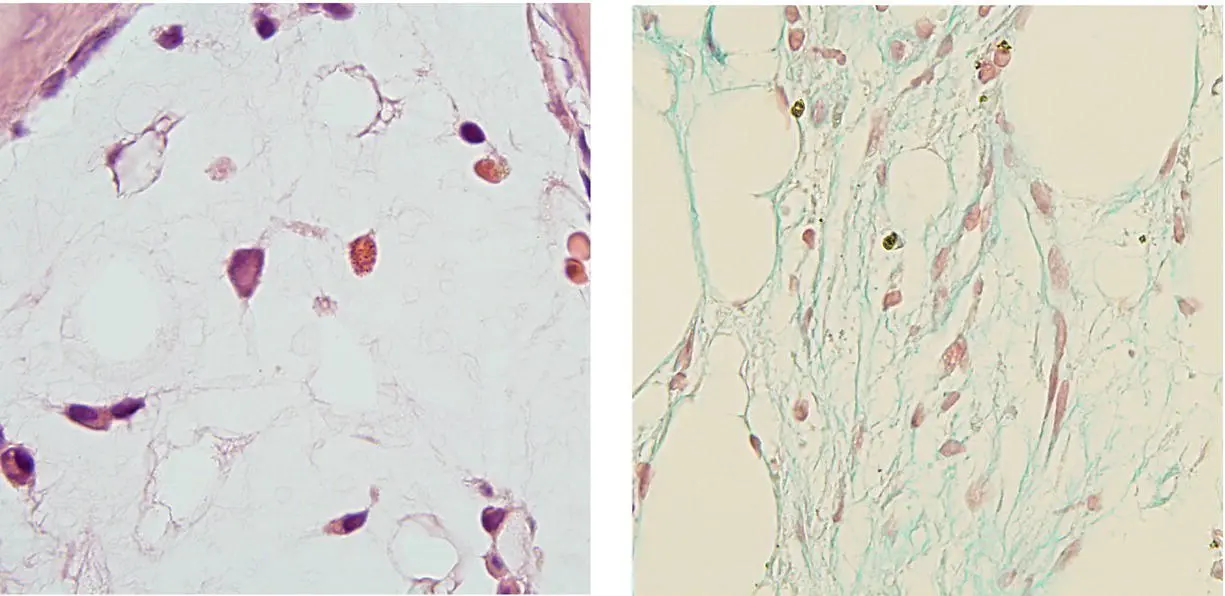
Typically, this condition involves the marrow diffusely (above left, H&E and right, Alcian blue ×50), resulting in peripheral blood cytopenias with neutropenia and anaemia being most frequent. Gelatinous transformation of the bone marrow is an important condition to recognise and should not be mistaken for marrow aplasia or marrow necrosis. It is typically seen as part of the catabolic response to chronic debilitating disease (malignant or non‐malignant) and/or malnutrition. The condition will regress on treating the underlying cause.
MCQ
1 Myxoid degeneration (gelatinous transformation) can be a feature of:Acquired immune deficiency syndromeAnorexia nervosaExtreme exerciseMetastatic carcinomaMorbid obesityFor answers and discussion, see page 206.
9 Acanthocytic red cell disorders
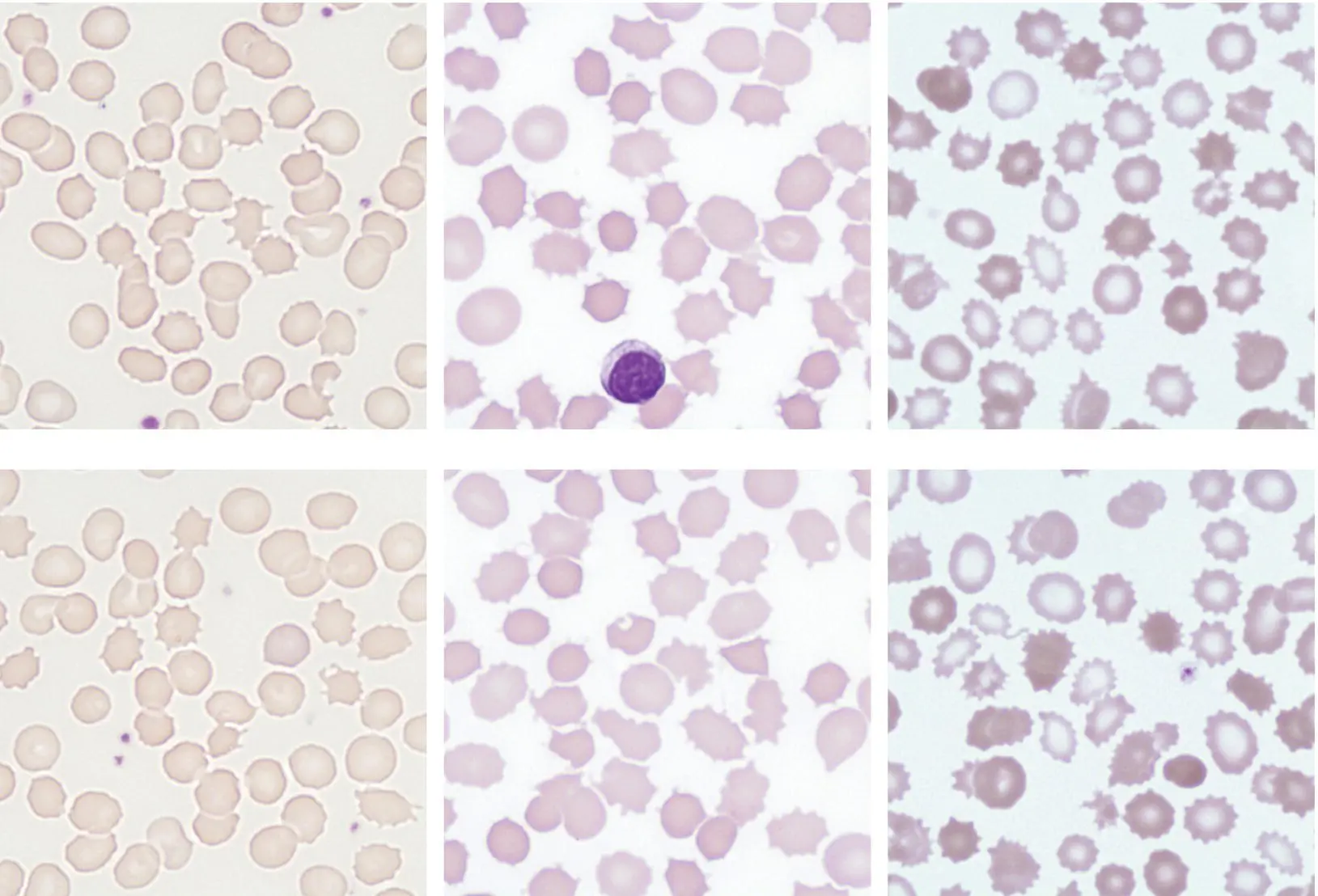
A 50‐year‐old man with a progressive myopathy and cardiomyopathy was referred to a neurologist because of early cognitive decline and tic‐like involuntary movements. His full blood count was normal but a blood film was requested. This showed prominent acanthocytes; these are dense cells with prominent cytoplasmic projections (spicules), which are irregular in length and shape ( acanthus is Greek for ‘thorny’) (left images ×100 objective). Routine renal and liver biochemistry and serum lipids were normal. A diagnosis of McLeod syndrome was considered and confirmed when a mutation in the XK gene at Xp21.1 was identified. McLeod syndrome is an X‐linked multisystem disorder, being one of a number of the rare neuroacanthocytic disorders. The condition is characterised by acanthocytosis, mild compensated haemolysis, weak expression of Kell blood group antigens, myopathy, cardiomyopathy and progressive neurological decline with cognitive impairment, involuntary movements, seizures and peripheral neuropathy. Peripheral blood morphology may provide a useful pointer to the diagnosis, as in this case.
A second patient, a 15‐year‐old boy was referred to ophthalmology with a progressive decline in visual acuity. He was found to have retinitis pigmentosa. He had a very low total cholesterol level, and low‐density and very low‐density lipoproteins (LDL and VLDL) were absent. His full blood count was normal but the requested blood film showed acanthocytes (centre images ×100). A diagnosis of abetalipoproteinaemia was considered and confirmed when biallelic mutation of the microsomal triglyceride transfer protein gene ( MTTP ) was identified. Abetalipoproteinaemia is a rare autosomal recessively inherited condition of lipid metabolism in which LDL and VLDL are severely reduced. The condition is characterised by fat malabsorption, spinocerebellar degeneration, acanthocytosis and retinitis pigmentosa. The MTTP protein influences intracellular lipid transport in the small bowel and liver. Symptoms usually first appear in infants and children, and when the condition is identified disease progression can be slowed using dietary vitamin E and medium chain fatty acid supplementation.
A third patient, a 32‐year‐old man with malnutrition from severe exocrine pancreatic insufficiency of unknown aetiology was hospitalised with a respiratory infection. He was poorly compliant with pancreatic enzyme supplements and appeared ill, grossly malnourished and wasted. His full blood count showed Hb 109 g/l, MCV 86.5 fl, MCH 26.3 pg, WBC 6.2 × 10 9/l and platelets 218 × 10 9/l. Serum ferritin was low at 9 μg/l and a blood film was requested. This showed significant hypochromia, consistent with iron deficiency, but also marked acanthocytosis with some of these cells appearing very dense (right images ×100). His lipid profile was abnormal, showing total cholesterol 2.2 mmol/l (optimal <5.2), triglycerides 0.8 mmol/l (NR 0.2–2.3), high‐density lipoprotein 0.6 mmol/l (optimal >1), LDL 1.2 mmol/l (optimal <2.59) and VLDL 0.4 mmol/l (NR 0.1–1.7). Serum apolipoprotein B levels were 0.6 g/l (NR 0.6–1.3) and screening for mutation in MTTP was negative. A diagnosis of acquired acanthocytosis, with iron deficiency secondary to severe lipid malabsorption from pancreatic exocrine failure was made.
MCQ
1 Acanthocytes in a blood film can be the result of:Anorexia nervosaLiver failureSplenectomyStorage artefactTransfusion of blood at the end of its shelf lifeFor answers and discussion, see page 206.
10 T‐cell large granular lymphocytic leukaemia
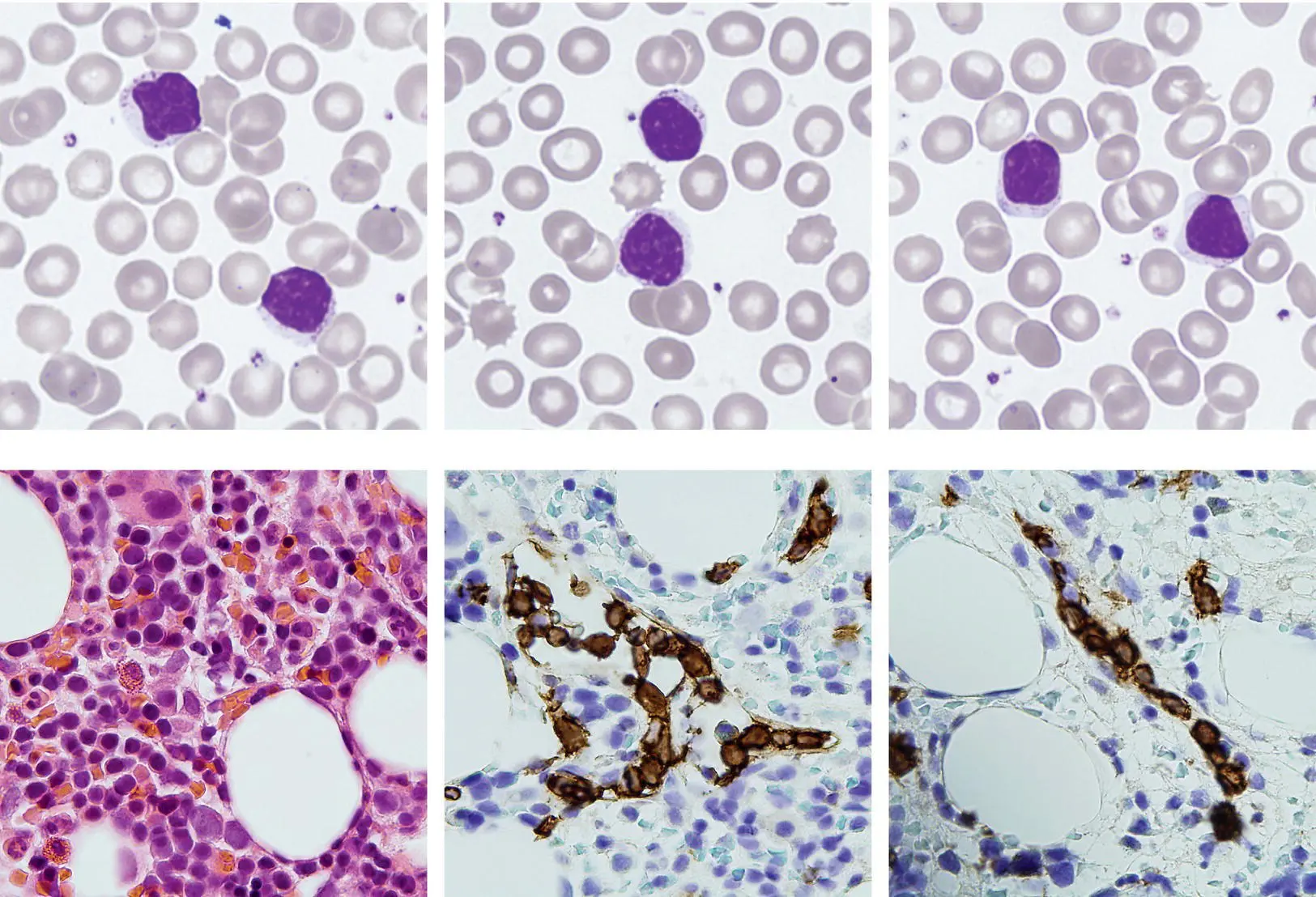
A 53‐year‐old man with rheumatoid arthritis was referred on account of progressive neutropenia whilst on weekly methotrexate therapy. Importantly, the methotrexate was withheld but the neutropenia continued and in fact worsened. At the time of referral the full blood count showed Hb 159 g/l, WBC 6.5 × 10 9/l, neutrophils 0.6 × 10 9/l, lymphocytes 5.1 × 10 9/l and platelets 133 × 10 9/l. The lymphocytosis had actually evolved during the period when methotrexate was suspended. The blood film showed prominent large granular lymphocytes (top images ×100 objective) and on immunophenotyping these expressed CD8, weak CD5, CD2, CD3 and CD57, whilst expression of CD7 and CD26 was lost, suggesting a clonal T‐cell disorder. The bone marrow trephine biopsy sections showed a cellular marrow with a subtle interstitial (bottom left, H&E ×50) and intrasinusoidal (CD3, bottom centre and right, immunoperoxidase ×50) T‐cell infiltrate. T‐cell receptor gene rearrangement studies showed a clonal population, and sequencing of STAT3 and STAT5B genes showed a gain of function mutation in STAT3 , Y640F, which has been associated with a therapeutic response to methotrexate. The clinical advice was therefore to restart methotrexate treatment. This resulted in improvement in rheumatic symptoms but also in resolution of lymphocytosis and neutropenia: Hb 160 g/l, WBC 5.0 × 10 9/l, neutrophils 2.1 × 10 9/l, lymphocytes 2.9 × 10 9/l and platelets 162 × 10 9/l.
Читать дальшеИнтервал:
Закладка:
Похожие книги на «Haematology»
Представляем Вашему вниманию похожие книги на «Haematology» списком для выбора. Мы отобрали схожую по названию и смыслу литературу в надежде предоставить читателям больше вариантов отыскать новые, интересные, ещё непрочитанные произведения.




Обсуждение, отзывы о книге «Haematology» и просто собственные мнения читателей. Оставьте ваши комментарии, напишите, что Вы думаете о произведении, его смысле или главных героях. Укажите что конкретно понравилось, а что нет, и почему Вы так считаете.