Innovations in Preventive Dentistry
Здесь есть возможность читать онлайн «Innovations in Preventive Dentistry» — ознакомительный отрывок электронной книги совершенно бесплатно, а после прочтения отрывка купить полную версию. В некоторых случаях можно слушать аудио, скачать через торрент в формате fb2 и присутствует краткое содержание. Жанр: unrecognised, на английском языке. Описание произведения, (предисловие) а так же отзывы посетителей доступны на портале библиотеки ЛибКат.

- Название:Innovations in Preventive Dentistry
- Автор:
- Жанр:
- Год:неизвестен
- ISBN:нет данных
- Рейтинг книги:5 / 5. Голосов: 1
-
Избранное:Добавить в избранное
- Отзывы:
-
Ваша оценка:
Innovations in Preventive Dentistry: краткое содержание, описание и аннотация
Предлагаем к чтению аннотацию, описание, краткое содержание или предисловие (зависит от того, что написал сам автор книги «Innovations in Preventive Dentistry»). Если вы не нашли необходимую информацию о книге — напишите в комментариях, мы постараемся отыскать её.
This book discusses new developments and innovations in preventive dentistry, from primary «real» prevention to secondary prevention by inactivating initial lesions, and on to tertiary prevention to avoid subsequent progression and
complications of manifest oral disease. This evidence base is then translated into clinical dental practice.
The book addresses everyone interested or involved in dentistry, including students, the whole dental practice team, educators, health scientists, and policy makers, who want to gain insight into these up-to-date clinical practices and future developments. It intends to make an impact on teaching and all fields of clinical dentistry – not by giving cookbook recipes, but by pointing out the rationale behind the changes in our routines.
Presented by an international group of recognized specialists in their fields, the topics include the new understanding and management of caries and periodontal disease, prevention of orthodontic problems, diagnostic approaches, the role of diet and according recommendations for oral health, routes to better oral hygiene, changes in oral disease patterns and their consequences, non- and minimally invasive caries treatment, current fluoride guidelines including the use of silver fluorides, risk management, a common risk-factor approach, facilitating behavior changes, sealants, and probiotics. This broad spectrum is elucidated for the most relevant dental problems from early childhood to seniors to implement preventively oriented dental practice.
Innovations in Preventive Dentistry — читать онлайн ознакомительный отрывок
Ниже представлен текст книги, разбитый по страницам. Система сохранения места последней прочитанной страницы, позволяет с удобством читать онлайн бесплатно книгу «Innovations in Preventive Dentistry», без необходимости каждый раз заново искать на чём Вы остановились. Поставьте закладку, и сможете в любой момент перейти на страницу, на которой закончили чтение.
Интервал:
Закладка:
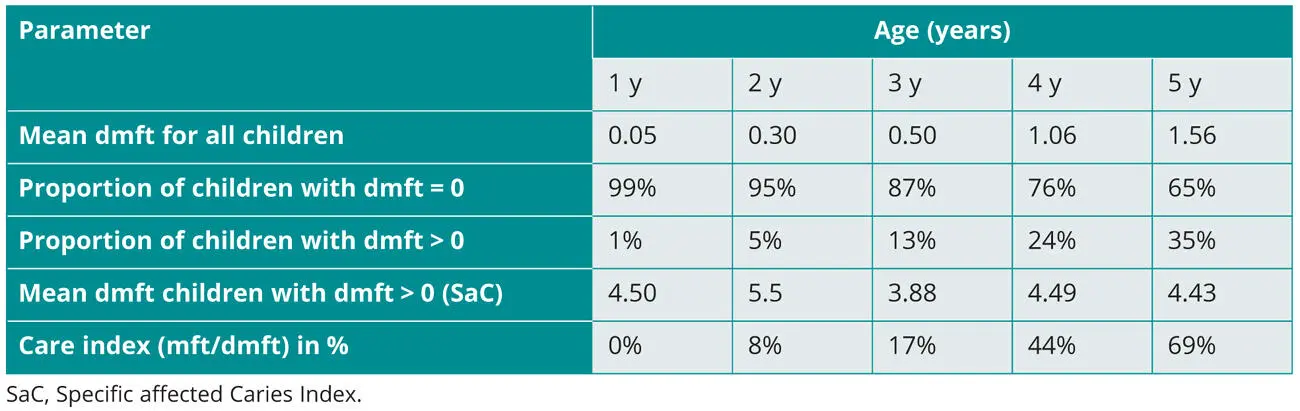
Table 1-1Mean caries prevalence data (dmft) for all kindergarten children in Greifswald, Germany, 2019, as well as mean values and care index for the subgroup of children with/without caries, fillings, and/or missing teeth due to caries (dmft = 0 and > 0, n ~ 1,500) 17
Caries diagnostics
Analogous to the above-mentioned definition of caries as a net loss of minerals, caries diagnostics would assess the change of minerals over time. As caries is a process, this implies that a one-time diagnosis requires a continuous sampling technique or is even per se impossible.
The ORCA/IADR consensus solves this problem by stating that “caries diagnosis is the clinical judgment integrating available information, including the detection and assessment of caries signs (lesions), to determine presence of the disease.” 1This is especially crucial for secondary or tertiary prevention, with the signs or symptoms of caries already being clearly present in an individual. “The main purpose of clinical caries diagnosis is to achieve the best health outcome for the patient by selecting the best management option for each lesion type, to inform the patient, and to monitor the clinical course of the disease.” 1This is relevant to all levels of prevention, as many teeth and surfaces within one individual often present different stages of the caries process.
It is important to comprehend that the diagnosis of caries as a process or caries activity differs from the diagnosis of past mineral loss or even cavitation, which was traditionally defined as “caries diagnostics.” According to ORCA/IADR, caries activity “is a concept that reflects the mineral balance, in terms of net mineral loss, net mineral gain, or stasis over time.” 1Caries active implies caries initiation or progression; caries inactive implies caries arrest or regression. 19The diagnosis of caries activity can actually be used as the gold standard for the success of preventive measures because they should reduce the net mineral loss to zero or even remineralize existing lesions. The detection of cavitation due to caries is a comparatively crude diagnostic approach.
Clinical examination
A regular, visual-tactile examination of the mouth and teeth is part of the standard routine in dentistry. However, active initial caries lesions, which are the crucial part of the diagnosis, can only be assessed clinically after removal of the dental plaque and drying of the teeth using sufficient lighting. It is important that no force is applied with a pointed probe during the examination of initial lesions, as this can destroy the intact surface and, therefore, reduce the chance of defect-free remineralization. 20
The International Caries Detection and Assessment System 21offers a detailed diagnosis of the various caries stages from 0 (healthy) to 6 (deep caries). In daily practice, however, it is usually sufficient in the diagnosis of caries to distinguish between healthy surfaces, initial lesions, moderate stage lesions, and cavitated lesions, as well as their degree of activity. 21-23
The clinical caries and activity diagnosis allows a fairly precise therapy decision and selection of the right level of care involving primary, secondary, or tertiary prevention. This makes the traditional concept of caries treatment obsolete. A merely restorative approach to caries would fail, as was often the case, due to the persisting net loss of minerals, leading to “secondary” caries, which is actually the nontreated caries activity that had originally led to the first cavitation.
Caries activity
The degree of caries activity is superior to the assessment of the caries risk (see Chapter 17). While risk refers to the conversion of a healthy state to disease, the diagnosis of caries activity actually uses the knowledge of the disease process to record its early signs, whether heavy plaque in stagnation areas, accompanying gingivitis, or initial caries lesion. These should be carefully viewed after cleaning and drying the teeth (Fig 1-5) and differentiated into a probably active or inactive initial lesion.
It is important to note that inactivation is possible at any stage from initial enamel lesion to deep dentinal caries (see Fig 1b), 21,23and it can be achieved by disturbing the dental biofilm (eg, by brushing teeth) and by influencing the de- and remineralization processes (eg, with fluorides). In spite of being classically primary preventive measures, they are “therapeutic” here and can be perceived as nonoperative caries treatment or management, which should result in a net gain of minerals.
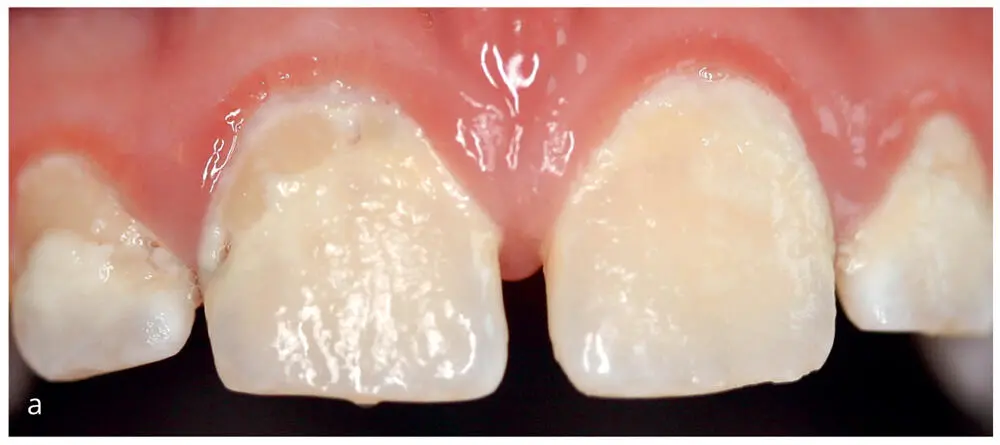
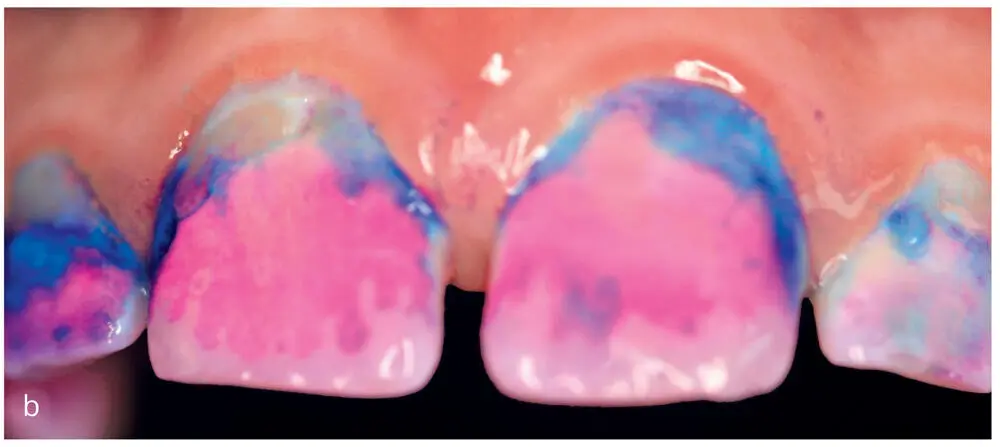
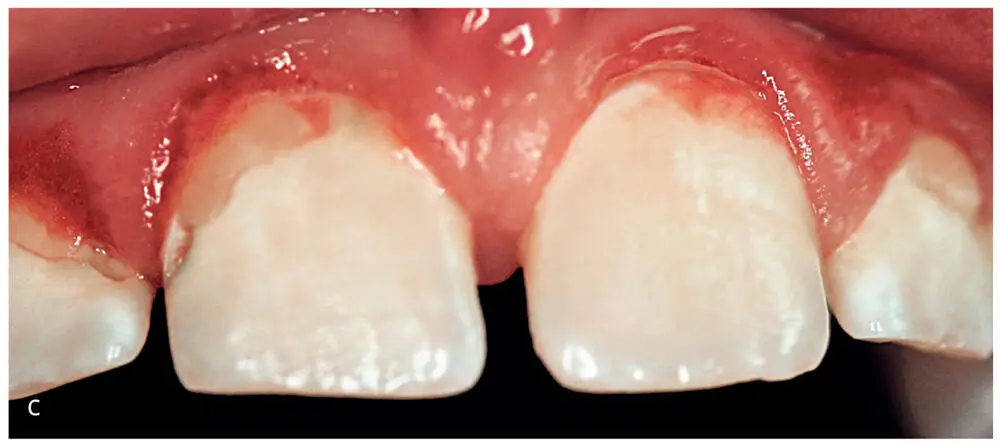
Figs 1-5a to cMaxillary anterior teeth: (a) before plaque removal, (b) after staining, and (c) after brushing. Active caries lesions can only be diagnosed on cleaned tooth surfaces, and gingivitis becomes clearer for the patient as a result of bleeding during cleaning.
Further diagnostics
If proximal caries is present or going to be expected, a radiographic examination should be considered since proximal caries rarely occurs in an isolated spot and pulpal involvement can be assessed (Fig 1-6). Bitewing radiographs are still considered to be the gold standard in proximal caries diagnostics. 24
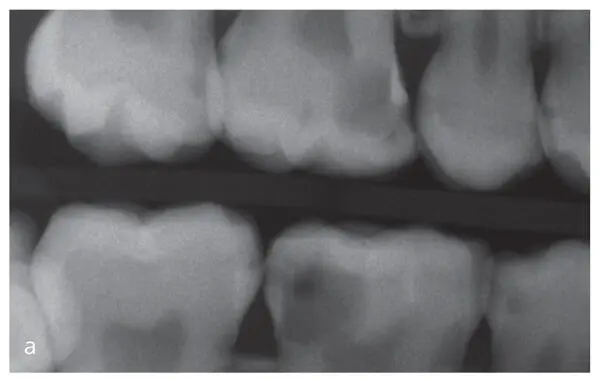

Figs 1-6a and bBitewing radiographs (a) allow a staging of proximal lesions and planning of primary preventive measures (flossing and fluorides, see Chapter 7), secondary prevention such as nonoperative treatment of initial lesions with cleaning and fluorides, proximal sealing or infiltration, and tertiary prevention meaning restorative care. This can be supported by fiber-optic transillumination (FOTI) (b), digital imaging fiber-optic transillumination (DIFOTI), or quantitative light-induced fluorescence (QLF).
Another method to monitor proximal surfaces is fiber-optic transillumination (FOTI), which is particularly suitable for the first examination of “apparently healthy” proximal surfaces, 25especially if a proximal lesion has already been detected on another tooth. In addition, several new caries diagnostic systems such as digital imaging fiber-optic transillumination (DIFOTI) and quantitative light-induced fluorescence (QLF) have been available on the market for several years with the aim of providing reliable results in caries diagnosis. Still, reviews stress that they can be used as adjunct tools, but they should not substitute x-rays completely, and do not overrule the clinical verification. 26
Current concepts and treatment approaches in caries management
Primary caries prevention is traditionally considered as the “real” prevention, aiming to maintain the health of sound teeth that are at risk for caries. The concepts of the classical preventive measures are based on a variety of approaches. In several chapters, this book looks at their current evidence base and provides clinical recommendations on how to implement these nowadays, eg for fluorides (see Chapter 3), plaque removal via tooth brushing or flossing (see Chapters 6and 7), diet control (see Chapter 4), or probiotics (see Chapter 11).
Читать дальшеИнтервал:
Закладка:
Похожие книги на «Innovations in Preventive Dentistry»
Представляем Вашему вниманию похожие книги на «Innovations in Preventive Dentistry» списком для выбора. Мы отобрали схожую по названию и смыслу литературу в надежде предоставить читателям больше вариантов отыскать новые, интересные, ещё непрочитанные произведения.







Обсуждение, отзывы о книге «Innovations in Preventive Dentistry» и просто собственные мнения читателей. Оставьте ваши комментарии, напишите, что Вы думаете о произведении, его смысле или главных героях. Укажите что конкретно понравилось, а что нет, и почему Вы так считаете.