Innovations in Preventive Dentistry
Здесь есть возможность читать онлайн «Innovations in Preventive Dentistry» — ознакомительный отрывок электронной книги совершенно бесплатно, а после прочтения отрывка купить полную версию. В некоторых случаях можно слушать аудио, скачать через торрент в формате fb2 и присутствует краткое содержание. Жанр: unrecognised, на английском языке. Описание произведения, (предисловие) а так же отзывы посетителей доступны на портале библиотеки ЛибКат.

- Название:Innovations in Preventive Dentistry
- Автор:
- Жанр:
- Год:неизвестен
- ISBN:нет данных
- Рейтинг книги:5 / 5. Голосов: 1
-
Избранное:Добавить в избранное
- Отзывы:
-
Ваша оценка:
Innovations in Preventive Dentistry: краткое содержание, описание и аннотация
Предлагаем к чтению аннотацию, описание, краткое содержание или предисловие (зависит от того, что написал сам автор книги «Innovations in Preventive Dentistry»). Если вы не нашли необходимую информацию о книге — напишите в комментариях, мы постараемся отыскать её.
This book discusses new developments and innovations in preventive dentistry, from primary «real» prevention to secondary prevention by inactivating initial lesions, and on to tertiary prevention to avoid subsequent progression and
complications of manifest oral disease. This evidence base is then translated into clinical dental practice.
The book addresses everyone interested or involved in dentistry, including students, the whole dental practice team, educators, health scientists, and policy makers, who want to gain insight into these up-to-date clinical practices and future developments. It intends to make an impact on teaching and all fields of clinical dentistry – not by giving cookbook recipes, but by pointing out the rationale behind the changes in our routines.
Presented by an international group of recognized specialists in their fields, the topics include the new understanding and management of caries and periodontal disease, prevention of orthodontic problems, diagnostic approaches, the role of diet and according recommendations for oral health, routes to better oral hygiene, changes in oral disease patterns and their consequences, non- and minimally invasive caries treatment, current fluoride guidelines including the use of silver fluorides, risk management, a common risk-factor approach, facilitating behavior changes, sealants, and probiotics. This broad spectrum is elucidated for the most relevant dental problems from early childhood to seniors to implement preventively oriented dental practice.
Innovations in Preventive Dentistry — читать онлайн ознакомительный отрывок
Ниже представлен текст книги, разбитый по страницам. Система сохранения места последней прочитанной страницы, позволяет с удобством читать онлайн бесплатно книгу «Innovations in Preventive Dentistry», без необходимости каждый раз заново искать на чём Вы остановились. Поставьте закладку, и сможете в любой момент перейти на страницу, на которой закончили чтение.
Интервал:
Закладка:
Kim R. Ekstrand, Azam Bakshandeh, Christian H. Splieth
Caries progression on occlusal surfaces
Preventive and therapeutically placed fissure sealants
Effectiveness of fissure sealants
Clinical application
From science to clinical recommendations
References
Chapter 11 – Prebiotics, probiotics, and synbiotics: A revolution in preventive dentistry?
Svante Twetman, Jukka H. Meurman, Egija Zaura
Oral prebiotics
Oral probiotics
Oral synbiotics
References
Chapter 12 – Silver fluorides: The new magic bullet?
Mohamed H. Abudrya, Christian H. Splieth, Ruth M. Santamaría
Historical background
Composition
Mechanism of action
Indications
Contraindications and side effects
Clinical application
Existing evidence
References
Chapter 13 – Self-assembling peptides: A perfectly engineered preventive and therapeutic tool?
Mohammad Alkilzy, Christian H. Splieth
Self-assembling peptide P11-4
In vitro studies
In vivo and clinical studies
Clinical application of P11-4 for treatment of initial caries
Further clinical implications of SAP
References
Chapter 14 – Nonrestorative cavity control: Can nonoperative “preventive” treatment replace restorations?
Ruth M. Santamaría, Nicola Innes
What is nonrestorative cavity control?
Natural history of dental caries
Prevention as a desirable approach to managing dental caries
Historical management of caries lesions
Is restorative management always necessary or possible?
How to carry out NRCC
What is the aim of NRCC?
For which patients is NRCC indicated?
NRCC technique
What are the main advantages of NRCC?
What are the main disadvantages of NRCC?
Is taking an NRCC approach cost-effective?
Is taking an NRCC approach clinically effective?
References
Chapter 15 – Prevention and prophylaxis in orthodontics: Neglected opportunities for successful prevention
Karl-Friedrich Krey, Anja Ratzmann, Nadezhda Stancheva
Etiology of malocclusion and malfunction as the basis of prevention
Form follows function
The beginning of orthodontic prevention
Breastfeeding, swallowing, and chewing
Habits and malfunctions
Playing musical instruments
Premature loss of primary molars and space maintainers
Canine retention
Unilateral reverse articulation
Anterior reverse articulation and periodontal health
Caries
Sleep disorders and upper airway management
Trauma prevention
Temporomandibular disorders
Third molar removal as prevention of crowding
Orofacial clefts
References
Chapter 16 – Prevention in elderly and medically compromised patients
Murali Srinivasan
Demographics of aging: related effects and retention of natural teeth
Periodontal disease and root caries
Prevention of periodontal disease
Prevention of root caries
References
Chapter 17 – Caries risk or activity: Which should we assess?
Margherita Fontana, Ruth M. Santamaría
Caries risk assessment
Caries activity
References
1
Understanding caries
Christian H. Splieth, Mhd Said Mourad, Mohammad Alkilzy, Julian Schmoeckel, Ruth M. Santamaría
In their new consensus statement on the terminology of dental caries and dental caries management, the European Organisation for Caries Research (ORCA) and the International Association for Dental Research (IADR) define caries as “a biofilm-mediated, diet modulated, multifactorial, noncommunicable, dynamic disease resulting in net mineral loss of dental hard tissues. It is determined by biologic, behavioral, psychosocial and environmental factors. As a consequence of this process, a caries lesion develops.” 1This very modern definition is based on the concept that caries is an imbalance of demineralization and remineralization that results from a dysbiosis of the oral biofilm, the overconsumption of carbohydrates, and insufficient oral hygiene (Fig 1-1).
Thus, the prevention of caries aims to adjust and ensure a healthy balance of the oral microbiome, dietary intake, oral hygiene, and mineral supply to avoid a net loss in enamel and dentin of healthy teeth. Caries therapy can only be successful in the long run if this is achieved when demineralization has already taken place. Therefore, caries prevention and its treatment employ the same concept and are nowadays combined as caries control, management, or care.

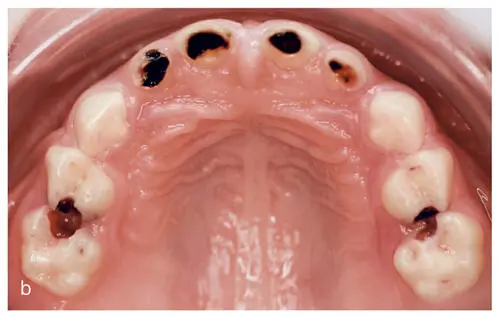
Figs 1-1a and bCaries is nowadays understood as an imbalance between de- and remineralizing factors resulting in a net loss of minerals (a). Thus, modern caries management modifies oral hygiene, diet, the biofilm, and the mineral equilibrium, keeping sound tooth surfaces healthy, inactivating existing caries lesions (b), and preventing recurrent demineralization around restorations.
This is also reflected in the ORCA/IADR definition of caries care, management, or control comprising “actions taken to interfere with mineral loss at all stages of the caries disease, including nonoperative and operative interventions/treatment. The terms caries care/management/control may be more appropriate than the term ‘caries prevention’ and because of the continuous de- and remineralization processes, caries control needs to be continued throughout the life course.” 1
In consequence, the terms of caries prevention and therapy merge, which is not really surprising as restorative care and accompanying efforts to reduce caries activity have been viewed as secondary and tertiary prevention for a long time. Taking this into account, ORCA/IADR state that caries prevention “traditionally meant inhibition of caries initiation, otherwise called primary prevention. Primary, together with secondary and tertiary prevention, comprising nonoperative and operative treatments, are now summarized under caries care, management, or control.” 1
The following chapters regarding caries risk prediction, fluoride use, biofilm and diet control, and promoting oral health are based on this new understanding of caries. As in periodontal disease, the primary goal of all preventive and therapeutic approaches is to achieve a high quality of life by establishing a physiologic, regenerative balance to maintain proper oral health.
Caries epidemiology and its consequences
On a global level, a remarkable caries decline could be achieved for the permanent dentition in children and adolescents in many industrialized regions such as the US, Canada, Europe, or Oceania. Although Germany was not the first country to experience this, consecutive and recent national surveys for all ages allow for a detailed analyses, which reveal trends 2,3that seem to be similar in many countries (Figs 1-2 and 1-3):
Caries prevalence has reduced from ten or more affected permanent teeth in adolescents during the 1970s to a mean of less than one decayed, missing, or filled teeth (DMFT) in 12-year-olds nowadays. 4
About 90% of the caries burden can be prevented and tooth loss is almost eradicated in the permanent dentition in adolescents. 2, 4
After the caries decline, 80% of the adolescents are caries-free on a DMFT level and this is not much changed by lowering the threshold to initial caries lesions. 3
Thus, the caries distribution is polarized and a so-called high-risk group of about 20% exhibits almost the complete caries burden. 2, 4
Читать дальшеИнтервал:
Закладка:
Похожие книги на «Innovations in Preventive Dentistry»
Представляем Вашему вниманию похожие книги на «Innovations in Preventive Dentistry» списком для выбора. Мы отобрали схожую по названию и смыслу литературу в надежде предоставить читателям больше вариантов отыскать новые, интересные, ещё непрочитанные произведения.







Обсуждение, отзывы о книге «Innovations in Preventive Dentistry» и просто собственные мнения читателей. Оставьте ваши комментарии, напишите, что Вы думаете о произведении, его смысле или главных героях. Укажите что конкретно понравилось, а что нет, и почему Вы так считаете.