Arun K Garg - Dermal Fillers for Dental Professionals
Здесь есть возможность читать онлайн «Arun K Garg - Dermal Fillers for Dental Professionals» — ознакомительный отрывок электронной книги совершенно бесплатно, а после прочтения отрывка купить полную версию. В некоторых случаях можно слушать аудио, скачать через торрент в формате fb2 и присутствует краткое содержание. Жанр: unrecognised, на английском языке. Описание произведения, (предисловие) а так же отзывы посетителей доступны на портале библиотеки ЛибКат.
- Название:Dermal Fillers for Dental Professionals
- Автор:
- Жанр:
- Год:неизвестен
- ISBN:нет данных
- Рейтинг книги:5 / 5. Голосов: 1
-
Избранное:Добавить в избранное
- Отзывы:
-
Ваша оценка:
Dermal Fillers for Dental Professionals: краткое содержание, описание и аннотация
Предлагаем к чтению аннотацию, описание, краткое содержание или предисловие (зависит от того, что написал сам автор книги «Dermal Fillers for Dental Professionals»). Если вы не нашли необходимую информацию о книге — напишите в комментариях, мы постараемся отыскать её.
Dermal Fillers for Dental Professionals — читать онлайн ознакомительный отрывок
Ниже представлен текст книги, разбитый по страницам. Система сохранения места последней прочитанной страницы, позволяет с удобством читать онлайн бесплатно книгу «Dermal Fillers for Dental Professionals», без необходимости каждый раз заново искать на чём Вы остановились. Поставьте закладку, и сможете в любой момент перейти на страницу, на которой закончили чтение.
Интервал:
Закладка:

FIG 2-7Locations for local anesthetic infiltration in preparation for basic dermal filler treatment.

FIG 2-8Locations for local anesthetic infiltration in preparation for advanced dermal filler treatment.
Local infiltration method
An 18-gauge, 1.5-inch needle is used to draw 1.0 mL buffered 2% lidocaine-epinephrine into a 1.0-mL syringe; the needle is then removed and replaced with a 30-gauge, 0.5-inch needle (unless otherwise directed). After the injection site has been cleaned with alcohol, 0.1 mL of the solution is injected at a time (Fig 2-9). Subsequent injections are administered on both sides of the face in accordance with the complexity of the site. Compression of the injected solution away from the treatment site can help reduce edema.


FIG 2-9 (a and b) Administration of local anesthetic for dermal filler injection in the tear trough region.
Ring blocks
Overview
Certain areas of facial dermal treatment, such as the lips and perioral region, are particularly sensitive to skin alteration when anesthesia is applied. To minimize or eliminate anesthesia distortion in these areas, many clinicians prefer the ring block administration method to achieve a stronger anesthesia effect using shorter, small-gauge needles. The gingivobuccal margin slightly beneath the submucosa is the typical injection site for lip ring blocks. However, if the treatment area requires the distal portions of the inferior branches of the infraorbital and mental nerves, the injections are made much deeper below the submucosa along the maxilla (for the infraorbital nerve) and mandible (for the mental nerve).
A total of 1.2 mL of buffered or unbuffered lidocaine 2% with epinephrine 1:100,000 solution is applied intraorally via four injections to establish the ring block in the lower or upper lip. Because it is more sensitive, the upper lip should be pretreated at the injection sites with a topical anesthetic gel such as 20% benzocaine. The corners of the lips are barely affected by such ring blocks; therefore, a single injection of 0.1 mL lidocaine-epinephrine solution should be administered in each corner (Fig 2-10).

FIG 2-10Ring block method for corners of lips. The white dots denote the locations where 0.1 mL lidocaine-epinephrine is injected.
Upper lip method
The patient should be placed in a 60-degree upright position, with the chin tilting upward. The upper lip is lifted to expose the gingivobuccal margin (Fig 2-11a). Topical benzocaine gel can be applied for 1 minute to anesthetize the injection points of the margin between the frenum and maxillary canines. A 30-gauge, 0.5-inch needle is inserted beneath the mucosa at an angle that is directed toward the pupil superiorly and parallel to the maxilla. Once the needle is advanced nearly its full length, 0.5 mL lidocaine solution is injected. If the solution does not flow smoothly, the needle may have been angled too superficially, placing the solution in the dermis. Once the needle is removed, the injected lidocaine should be compressed superiorly, toward the infraorbital foramen.
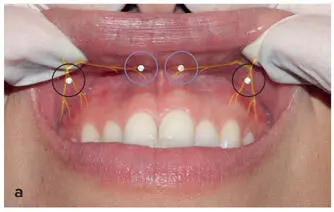


FIG 2-11 (a to c) Ring block method for upper lip. The black circles denote the locations where 0.5 mL lidocaine-epinephrine is injected, and the blue circles denote the locations where 1.0 mL lidocaine-epinephrine is injected.
Next, local infiltration is applied to the corners of the lips (Figs 2-11b and 2-11c). In each corner, the needle tip is inserted slightly beneath the mucosa, and 0.1 mL lidocaine is injected, followed by compression. The clinician then moves to the opposite side of the patient and repeats the injections previously made contralaterally. A period of 5 to 10 minutes is usually sufficient for the anesthesia to take effect. Absence of sensation should be confirmed before the dermal filler procedure is initiated. An additional 0.5 mL of anesthetic solution can be administered at the maxillary canine injection site.
Lower lip method
As with the upper lip ring block, the patient should be placed in a 60-degree upright position with the chin tilting upward. The lower lip is lifted to expose the gingivo-buccal margin slightly lateral to the mandibular first premolar (Fig 2-12a). This time, the needle is directed toward the mental foramen, parallel to the mandible, and the same precautions against superficial injection should be exercised as in the upper lip area. Compression of the lidocaine solution, this time toward the mental foramen, should be applied after the injection. Next, a second injection is made slightly lateral to the frenulum of the lower lip (Figs 2-12b and 2-12c). The tip of the needle is inserted just beneath the mucosa, and 0.1 mL of the solution is injected, followed by compression of the site once the needle is removed.
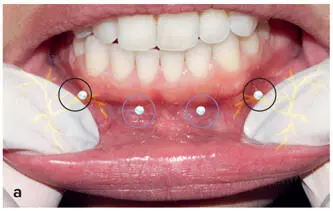


FIG 2-12 (a to c) Ring block method for lower lip. The black circles denote the locations where 0.5 mL lidocaine-epinephrine is injected, and the blue circles denote the locations where 1.0 mL lidocaine-epinephrine is injected.
The clinician then moves to the opposite side of the patient and repeats the injections for the contralateral side of the lower lip. Additional lidocaine can be applied at the mandibular first premolar if needed.
Conclusion
Local anesthesia is a critical component of an esthetic practice just as it is a dental practice. Although they do not receive formal training in esthetic dermal filler treatment in dental school, dentists have extensive experience in pain control and are experts on the musculature and anatomy of the face. Most dentists will find this knowledge invaluable for mastering the various methods of administering anesthesia prior to dermal filler treatment, some of which they perform in their everyday dental practices.
Читать дальшеИнтервал:
Закладка:
Похожие книги на «Dermal Fillers for Dental Professionals»
Представляем Вашему вниманию похожие книги на «Dermal Fillers for Dental Professionals» списком для выбора. Мы отобрали схожую по названию и смыслу литературу в надежде предоставить читателям больше вариантов отыскать новые, интересные, ещё непрочитанные произведения.







Обсуждение, отзывы о книге «Dermal Fillers for Dental Professionals» и просто собственные мнения читателей. Оставьте ваши комментарии, напишите, что Вы думаете о произведении, его смысле или главных героях. Укажите что конкретно понравилось, а что нет, и почему Вы так считаете.