Essential Cases in Head and Neck Oncology
Здесь есть возможность читать онлайн «Essential Cases in Head and Neck Oncology» — ознакомительный отрывок электронной книги совершенно бесплатно, а после прочтения отрывка купить полную версию. В некоторых случаях можно слушать аудио, скачать через торрент в формате fb2 и присутствует краткое содержание. Жанр: unrecognised, на английском языке. Описание произведения, (предисловие) а так же отзывы посетителей доступны на портале библиотеки ЛибКат.
- Название:Essential Cases in Head and Neck Oncology
- Автор:
- Жанр:
- Год:неизвестен
- ISBN:нет данных
- Рейтинг книги:5 / 5. Голосов: 1
-
Избранное:Добавить в избранное
- Отзывы:
-
Ваша оценка:
Essential Cases in Head and Neck Oncology: краткое содержание, описание и аннотация
Предлагаем к чтению аннотацию, описание, краткое содержание или предисловие (зависит от того, что написал сам автор книги «Essential Cases in Head and Neck Oncology»). Если вы не нашли необходимую информацию о книге — напишите в комментариях, мы постараемся отыскать её.
Essential Cases in Head and Neck Oncology This textbook also includes:
Covers the full spectrum of head and neck surgeries, including reconstructive procedures Discusses ethics related to cancer treatments, medical research, and other care issues Promotes multidisciplinary critical thinking, clinical problem-solving, communication, and collaboration Helps medical students and trainees evaluate their learning and contextualize their knowledge Features high-quality images and succinct explanatory text throughout
is an indispensable study aid for trainee clinicians, residents, and fellows studying for board certification and other exams, and an excellent reference guide for oncologists, otolaryngologists, surgeons, and other practitioners working in medical oncology, radiation oncology, and oromaxillofacial surgery.
Essential Cases in Head and Neck Oncology — читать онлайн ознакомительный отрывок
Ниже представлен текст книги, разбитый по страницам. Система сохранения места последней прочитанной страницы, позволяет с удобством читать онлайн бесплатно книгу «Essential Cases in Head and Neck Oncology», без необходимости каждый раз заново искать на чём Вы остановились. Поставьте закладку, и сможете в любой момент перейти на страницу, на которой закончили чтение.
Интервал:
Закладка:
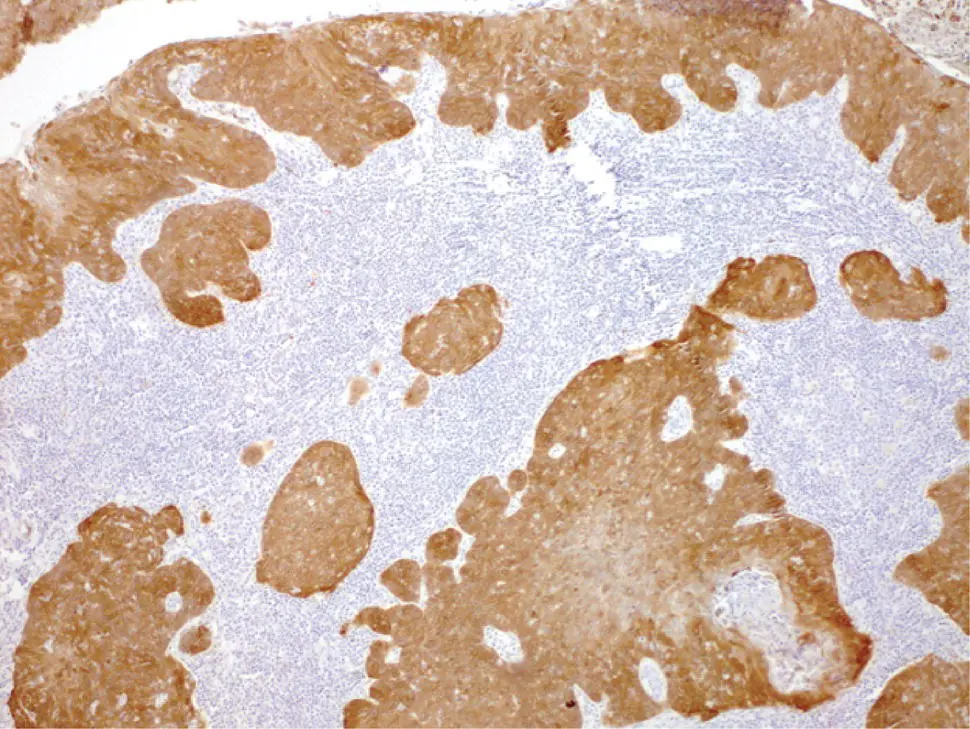
FIGURE 9.4 Histologic images of a poorly differentiated squamous cell carcinoma with >70% nuclear and cytoplasmic staining for p16.
Question: What is the most appropriate stage assignment?
Answer:cT1N1M0, prognostic stage I. The demographics of patients affected by p16+ OPSCC are distinct from those affected by p16 negative OPSCC. Patients affected by p16+ OPSCC are often younger, have limited or no exposure to tobacco and alcohol, and have fewer comorbidities compared to patients affected by p16 negative disease. These tumors also are significantly more responsive to radiotherapy. As a result, the prognosis of patients with p16+ OPSCC is markedly better. A study by Ang et al. (2010) highlighted that tumor HPV status is a strong, independent prognostic factor for survival in OPSCC (3‐year overall survival for patients with HPV‐positive tumors was 82.4% vs. 57.1% for patients with HPV‐negative tumors, P < 0.001, and HPV‐positive tumors were associated with a 58% reduction in the risk of death [hazard ratio, 0.42; 95% CI, 0.27 to 0.66]). This distinct, favorable prognostic behavior has been recognized in the creation of a separate staging system specific to p16+ OPSCC, which reorganizes the TNM classification and prognostic stage grouping. As a result, a patient with a p16+ T1 or T2 primary neoplasm, and ipsilateral lymph node involvement <6 cm in greatest dimension (irrespective of number of nodes), and no distant metastases, is classified as cT1N1M0, and assigned prognostic stage I.
Question: What is/are the appropriate treatment recommendations for this patient?
Answer:Patients with p16+ OPSCC with small primary neoplasms (T1–2) and single ipsilateral lymph node ≤3 cm, without adverse features on pathology may be treated using single modality treatment (surgery or radiotherapy). It is important to recognize that while there is significant interest in de‐escalation of therapy to minimize treatment‐related morbidity, especially in the context of expected favorable prognosis in patients affected by p16+ OPSCC, any efforts toward de‐escalation should be pursued strictly in the context of clinical trials. The treatment algorithms are best determined by extent and burden of disease, and not on the basis of revised prognostic groups that have been newly assigned to this unique disease.
Key Points
Surgical treatment of oropharyngeal carcinoma is appropriate in patients with transorally accessible early‐stage cancers without pathologically concerning features and no more than one ipsilateral lymph node.
Surgical treatment of oropharyngeal carcinoma can be done through transoral traditional, laser and robotic techniques. Patient factors such as trismus or having a narrow mandible or torus mandibularis may limit exposure. Moreover, a retropharyngeal internal carotid artery is a contraindication for transoral surgery for tumors involving the palatine tonsils.
Patients with obvious indications for postoperative chemoradiation should be given strong consideration for treatment with nonsurgical means to avoid trimodality therapy and reduce treatment burden.
Ipsilateral versus bilateral neck dissection depends on the location of the oropharyngeal tumor. Tumors limited to the palatine tonsil can be managed with ipsilateral dissection, whereas base of tongue cancers or those with significant soft palate extension should be considered for bilateral treatment.
CASE 10
Daniel Sharbel and Kenneth Byrd
History of Present Illness
A 67‐year‐old Caucasian male with a history of cT2N1M0 SCC of the right tongue base treated with chemoradiation 3 years ago presented to his primary care physician complaining of several weeks of severe pain in his right upper neck, right cheek, and ear.
Past Medical History
Coronary artery disease with history of stenting 2 years prior, and peripheral vascular disease.
Nonsmall‐cell lung cancer treated with chemoradiation therapy fifteen years ago.
Past Surgical History
History of prior cervical spine surgery.
Social History
Former smoker with 40 pack‐year history, quit more than 20 years ago. Former drinker, quit more than 20 years ago.
Question: What additional questions would you want to ask?
Any trouble swallowing? Yes.
Any recent infection? Patient Denies.
Any hemoptysis or hematemesis? Patient Denies.
Any difficulty opening and closing the mouth? Patient denies.
Any other masses in the neck that have been noticed? Patient denies.
Any sexually transmitted diseases? None known. The presence of these may increase likelihood of HPV exposure.
History of tracheostomy or gastrostomy? Patient denies. The presence of these may suggest dependence postoperatively.
Performance status? ECOG 1.
Physical Examination
Thin, adult male in mild distress from pain but breathing comfortably.
Skin: no suspicious lesions.
Oral cavity and oropharynx: 3 cm right‐sided nodular tumor arising from the tonsillar bed.
Neck: cervical exam reveals no palpable lymphadenopathy or salivary lesions.
Cranial nerves II–XII intact.
Flexible fiberoptic laryngoscopy: large right tonsillar mass. The epiglottis is displaced inferiorly and posteriorly on exam. The view of the glottis is limited but without any apparent involvement, and the true vocal folds are bilaterally mobile.
Contrasted CT of the neck was performed (see Figure 10.1).
Question: What is the next appropriate step in management?
Answer:Histopathologic diagnostic confirmation is recommended prior to proceeding with next steps in treatment. In this instance, this can likely be performed via a transoral office biopsy. If exposure is a challenge and/or there are concerns for significant bleeding due to the tumor appearance or a patient being on anticoagulation, a panendoscopy under general anesthesia could be performed.
Biopsy confirms diagnosis of SCC, p16 negative.
Question: Are any further imaging studies appropriate?
PET/CT: yes/no. This is an ideal imaging study as it will reveal the extent of the recurrence, evaluate for regional and distant disease, and assess for a second primary lesion. FIGURE 10.1 AxialAxial CT image. FIGURE 10.2 18FDG‐PET/CT axial view demonstrating an intense right tonsil tumor with an SUV of 16.6. No regional or distant lesions were noted.
MRI neck: yes/no. MRI can provide increased soft tissue detail when evaluating cancers of the oropharynx. This may be particularly beneficial in this case when assessing for parapharyngeal space extension. Evaluation for retropharyngeal lymphadenopathy is also important. An MRI is unlikely to yield more information in this patient that will alter management compared with the information available from the CT neck with contrast. Although not strictly contraindicated its value is limited in this patient.
Ultrasound: yes/no. This study is not indicated because given the location of the primary tumor adjacent to the mandible, the bone would preclude complete evaluation of the primary cancer.
Chest CT: yes/no. If a PET scan is not obtained, a chest CT would be helpful to assess for distant disease or a recurrence of his lung cancer.
An 18FDG‐PET/CT was performed from skull base to midthigh (see Figure 10.2) due to the recurrent oropharyngeal cancer, as well as the history of lung cancer. The patient was then presented at a multidisciplinary tumor board.
Читать дальшеИнтервал:
Закладка:
Похожие книги на «Essential Cases in Head and Neck Oncology»
Представляем Вашему вниманию похожие книги на «Essential Cases in Head and Neck Oncology» списком для выбора. Мы отобрали схожую по названию и смыслу литературу в надежде предоставить читателям больше вариантов отыскать новые, интересные, ещё непрочитанные произведения.





Обсуждение, отзывы о книге «Essential Cases in Head and Neck Oncology» и просто собственные мнения читателей. Оставьте ваши комментарии, напишите, что Вы думаете о произведении, его смысле или главных героях. Укажите что конкретно понравилось, а что нет, и почему Вы так считаете.