Essential Cases in Head and Neck Oncology
Здесь есть возможность читать онлайн «Essential Cases in Head and Neck Oncology» — ознакомительный отрывок электронной книги совершенно бесплатно, а после прочтения отрывка купить полную версию. В некоторых случаях можно слушать аудио, скачать через торрент в формате fb2 и присутствует краткое содержание. Жанр: unrecognised, на английском языке. Описание произведения, (предисловие) а так же отзывы посетителей доступны на портале библиотеки ЛибКат.
- Название:Essential Cases in Head and Neck Oncology
- Автор:
- Жанр:
- Год:неизвестен
- ISBN:нет данных
- Рейтинг книги:5 / 5. Голосов: 1
-
Избранное:Добавить в избранное
- Отзывы:
-
Ваша оценка:
Essential Cases in Head and Neck Oncology: краткое содержание, описание и аннотация
Предлагаем к чтению аннотацию, описание, краткое содержание или предисловие (зависит от того, что написал сам автор книги «Essential Cases in Head and Neck Oncology»). Если вы не нашли необходимую информацию о книге — напишите в комментариях, мы постараемся отыскать её.
Essential Cases in Head and Neck Oncology This textbook also includes:
Covers the full spectrum of head and neck surgeries, including reconstructive procedures Discusses ethics related to cancer treatments, medical research, and other care issues Promotes multidisciplinary critical thinking, clinical problem-solving, communication, and collaboration Helps medical students and trainees evaluate their learning and contextualize their knowledge Features high-quality images and succinct explanatory text throughout
is an indispensable study aid for trainee clinicians, residents, and fellows studying for board certification and other exams, and an excellent reference guide for oncologists, otolaryngologists, surgeons, and other practitioners working in medical oncology, radiation oncology, and oromaxillofacial surgery.
Essential Cases in Head and Neck Oncology — читать онлайн ознакомительный отрывок
Ниже представлен текст книги, разбитый по страницам. Система сохранения места последней прочитанной страницы, позволяет с удобством читать онлайн бесплатно книгу «Essential Cases in Head and Neck Oncology», без необходимости каждый раз заново искать на чём Вы остановились. Поставьте закладку, и сможете в любой момент перейти на страницу, на которой закончили чтение.
Интервал:
Закладка:
The use of pembrolizumab is indicated in unresectable locoregionally recurrent head and neck cancer and/or distant metastatic disease. Its mechanism is to bind to the PD‐1 receptors on lymphocytes to disrupt the local immune‐suppression generated by the cancer. The use of immunotherapy in the primary treatment of cancer is an area of active investigation.
Following definitive chemoradiation therapy, a post‐treatment PET/CT was performed 12 weeks after completion of treatment showing no evidence of local, regional or distant disease. The patient was started on regular surveillance follow‐up with visits every 3 months.
Key Points
The presence of trismus in a patient with an oropharyngeal carcinoma reflects either perineural invasion or direct extension to the pterygoid muscles. The presence of either would predict aggressive behavior.
It is important to completely and accurately assess a patient for surgical resectability prior to undertaking a surgical approach. A large tumor at risk of excision with positive margins obligates the patient to receive trimodality therapy if surgery is pursued.
If there is concern regarding resectability, the patient is best treated nonoperatively to decrease morbidity.
PET/CT after chemoradiation therapy must be obtained at least 12 weeks after completion of treatment to allow for accurate assessment of treatment response.
A negative PET/CT at the completion of therapy is a reliable predictor of a complete response.
Platinum‐based chemotherapy is the mainstay of head and neck SCC treatment, but there are other effective options for those patients who cannot receive platinum‐based agents.
CASE 9
Aru Panwar
History of Present Illness
A 52‐year‐old man who works on a farm presents with an asymptomatic right upper neck mass for 6 weeks.
Question: What additional questions would you want to ask?
Is it painful? Patient denies.
Is it tender to the touch? Patient denies.
Is it growing? Patient denies.
Any trouble swallowing? Patient denies.
Any voice changes? Patient denies.
Any throat pain? Patient denies.
Any ear pain? Patient denies.
Any skin changes over the mass? Patient denies. Erythema or induration could indicate extranodal extension of a malignancy or an infectious etiology (e.g., scrofula).
Has he received any treatment for this? Patient denies.
Past Medical History
None.
Past Surgical History
None.
Social History
Nonsmoker.
Physical Examination
Well‐developed male in no distress. Voice strong.
Skin: no suspicious lesions.
Oral cavity examination shows teeth in good condition. No lesions seen or palpated.
Oropharynx: slight fullness of the right tonsil. Difficult to palpate due to gag reflex.
Cervical exam: firm, 3 cm right level IIA neck mass that is mobile on palpation. Salivary gland exam is normal. No other neck masses.
Cranial nerves II–XII intact.
Flexible laryngoscopy is performed and is pictured below (see Figure 9.1).
Management
Question: Which of the following would be appropriate options in the management of this patient?
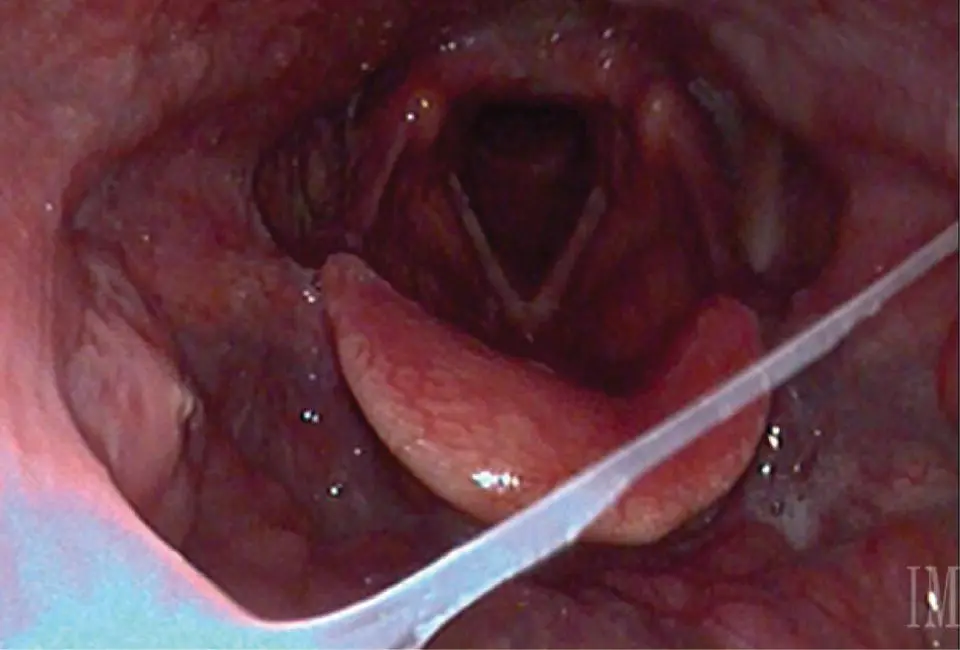
FIGURE 9.1 This image from a transnasal fiberoptic laryngoscopy shows no obvious primary lesion. The true vocal folds are fully mobile, bilaterally.
CT with contrast or MRI: yes/no. A contrast‐enhanced CT or MRI of the neck should also be ordered to characterize the suspected primary neoplastic site, identify regional anatomy and extent of regional nodal disease. CT allows for rapid image acquisition with less motion artifact and also evaluates for bone erosion (see Figure 9.2). MRI provides improved soft tissue detail for tumors with deep tongue and/or parapharyngeal space extension and also may be helpful in identifying perineural invasion.
Fine needle aspiration of neck mass: yes/no. Determination of etiology may hinge on cytologic identification of malignancy through fine needle aspiration of an enlarged lymph node. Fine needle aspiration is safe, cost‐effective, and highly accurate (sensitivity 89.6%, specificity 96.5%, positive predictive value 96.2%, and negative predictive value 90.3%).
PET/CT imaging: yes/no. A PET/CT may be requested in appropriately selected patients after a diagnosis of malignancy has been established as it may help guide the workup for the primary lesion. It is primarily indicated in patients with significant cervical nodal disease and/or in those patients with no identifiable primary lesion (see Figure 9.3).
Antibiotic treatment for 2 weeks, followed by repeat examination: yes/no. A persistent neck mass in older adults that persists for greater than 2 weeks or is of uncertain duration should raise significant concern for underlying malignancy. Other concerning features associated with the presentation include absence of infectious etiology, firm consistency, neck mass >1.5 cm, and tonsil asymmetry. Patients who present with neck masses and high suspicion for underlying malignancy should not be routinely offered antibiotics unless there are signs and symptoms of bacterial infection. FIGURE 9.2 A contrast‐enhanced CT of the neck demonstrates a solitary, enlarged, partially cystic right level II cervical lymph node. CT exam of the oropharynx is obscured by dental artifact. FIGURE 9.3 A PET/CT demonstrates no distant metastatic sites but shows focal uptake in the right palatine tonsil and in the solitary right level II cervical lymph node.
Open incisional biopsy of right neck mass: yes/no. Incisional biopsy of neck masses should be avoided in favor of fine needle aspiration. In some circumstances, an excisional biopsy of a neck mass may be considered when diagnosis remains elusive despite appropriate clinical examination, imaging, fine needle aspiration cytology, comprehensive examination under anesthesia, and biopsy of alternative sites including sites suspected to harbor a primary neoplasm do not provide a definitive diagnosis. If an open biopsy is needed, the patient should also be consented for a neck dissection if the frozen section shows carcinoma.
A fine needle aspiration of the neck mass reveals the diagnosis of SCC with basaloid appearing cells in a background of necrosis.
Question: What is the next appropriate ancillary test for this patient?
Answer:p16 expression tested by IHC is widely available, cost‐sensitive and a reliable surrogate for HPV status (sensitivity 94–97%, specificity 83–84%). The AJCC 8th Edition uses p16 status as the agreed upon biomarker to determine TNM class and prognostic stage grouping specific to HPV‐associated oropharyngeal SCCs (OPSCC). Distinction between p16 posi tive (defined as >70% nuclear and cytoplasmic staining on IHC) and p16 negative OPSCC is critical to choosing the appropriate staging schema and determination of prognosis. The p16 IHC and polymerase chain reaction (PCR)‐based assays have high sensitivity, although ISH boasts the highest specificity. Epstein–Barr virus testing should be considered for patients presenting with suspected nasopharyngeal carcinoma and patients with unknown primary site where nasopharyngeal malignancy is part of the differential diagnosis.
This Patient undergoes panendoscopy and biopsy from tonsil reveals invasive SCC.
IHC test for p16 suggests >70% positive nuclear and cytoplasmic staining ( Figure 9.4). On palpation in the OR, the tumor lesion is limited to the tonsil and the base of tongue is soft and without evidence of tumor. A biopsy of the base of tongue adjacent to the tonsil primary is negative for carcinoma.
Читать дальшеИнтервал:
Закладка:
Похожие книги на «Essential Cases in Head and Neck Oncology»
Представляем Вашему вниманию похожие книги на «Essential Cases in Head and Neck Oncology» списком для выбора. Мы отобрали схожую по названию и смыслу литературу в надежде предоставить читателям больше вариантов отыскать новые, интересные, ещё непрочитанные произведения.





Обсуждение, отзывы о книге «Essential Cases in Head and Neck Oncology» и просто собственные мнения читателей. Оставьте ваши комментарии, напишите, что Вы думаете о произведении, его смысле или главных героях. Укажите что конкретно понравилось, а что нет, и почему Вы так считаете.