Pathy's Principles and Practice of Geriatric Medicine
Здесь есть возможность читать онлайн «Pathy's Principles and Practice of Geriatric Medicine» — ознакомительный отрывок электронной книги совершенно бесплатно, а после прочтения отрывка купить полную версию. В некоторых случаях можно слушать аудио, скачать через торрент в формате fb2 и присутствует краткое содержание. Жанр: unrecognised, на английском языке. Описание произведения, (предисловие) а так же отзывы посетителей доступны на портале библиотеки ЛибКат.
- Название:Pathy's Principles and Practice of Geriatric Medicine
- Автор:
- Жанр:
- Год:неизвестен
- ISBN:нет данных
- Рейтинг книги:3 / 5. Голосов: 1
-
Избранное:Добавить в избранное
- Отзывы:
-
Ваша оценка:
Pathy's Principles and Practice of Geriatric Medicine: краткое содержание, описание и аннотация
Предлагаем к чтению аннотацию, описание, краткое содержание или предисловие (зависит от того, что написал сам автор книги «Pathy's Principles and Practice of Geriatric Medicine»). Если вы не нашли необходимую информацию о книге — напишите в комментариях, мы постараемся отыскать её.
Pathy’s Principles and Practice of Geriatric Medicine
Pathy's Principles and Practice of Geriatric Medicine — читать онлайн ознакомительный отрывок
Ниже представлен текст книги, разбитый по страницам. Система сохранения места последней прочитанной страницы, позволяет с удобством читать онлайн бесплатно книгу «Pathy's Principles and Practice of Geriatric Medicine», без необходимости каждый раз заново искать на чём Вы остановились. Поставьте закладку, и сможете в любой момент перейти на страницу, на которой закончили чтение.
Интервал:
Закладка:
| Myeloproliferative syndromes |
| Myelodysplasia |
| Uraemia |
| Cardiopulmonary bypass |
Similarly, in myelodysplastic syndromes, in addition to frequent thrombocytopenia, abnormal platelet function is common, and bleeding can cause severe morbidity requiring platelet transfusion; bleeding and infection are the most common causes of death. Abnormalities of platelet function leading to a prolonged bleeding time frequently occur in uraemia. This improves with dialysis and can be specifically treated, if necessary, with desmopressin (DDAVP). Due primarily to proteolytic degradation of platelet surface glycoproteins by plasma, an acquired platelet function defect occurs during extracorporeal circulation in cardiopulmonary bypass. It can be ameliorated by using the fibrinolytic inhibitor aprotinin but may also require platelet transfusion. Congenital functional platelet defects are extremely rare, with an incidence of less than one per million of the population. Deficiency of the platelet‐specific glycoprotein Ib, which allows interaction with the von Willebrand factor, occurs in Bernard–Soulier syndrome; and deficiency of the platelet surface glycoprotein IIb/IIIa occurs in Glanzmann’s thrombasthenia. Deficiency of platelet alpha and dense granules, which are usually released upon platelet aggregation and are involved in the recruitment of large numbers of platelets into the platelet plug, are deficient in storage pool disease. 6
Hereditary coagulation defects
Severe deficiency ( < 0.01 IU/ml) of factor VIII (haemophilia A) or factor IX (haemophilia B) will have been diagnosed at a young age, and management of these conditions is highly specialized and age‐independent. Spontaneous bleeding into muscles and joints is frequent and is managed by infusions of appropriate clotting factor concentrates ( Figure 24.1). In addition, many older patients have severe complications of advanced haemophiliac arthropathy and often hepatic impairment due to chronic infection with hepatitis viruses, especially hepatitis C virus but also chronic hepatitis B. Both types of hepatitis can now be successfully treated. Haemophilia A and B both have gender‐linked inheritance and occur in males. Mild ( > 0.05 IU/ml) and moderate (0.01–0.05 IU/ml) cases may have escaped diagnosis until a later age and will not present until they have a severe haemostatic challenge such as surgery, which can occur at any age. These patients will have a long APTT, and specific factor assays will reveal the diagnosis. Patients with mild haemophilia A can usually be managed with desmopressin, a long‐acting synthetic analogue of vasopressin, the antidiuretic hormone, rather than with clotting factor concentrates, with the attendant cost savings and reduced risk of viral transmission. Female carriers of haemophilia A and B usually have around half the normal levels of the respective clotting factor, although, owing to the randomness of the lyonization effect (random inactivation of one X chromosome in all female cells), up to 30% of carriers have factor VIII or factor IX levels sufficiently low to require treatment at times of surgery. Conversely, many carriers have entirely normal levels of factor VIII and factor IX; therefore, carrier status cannot be determined accurately simply by measuring the appropriate factor levels but instead requires genetic analysis.
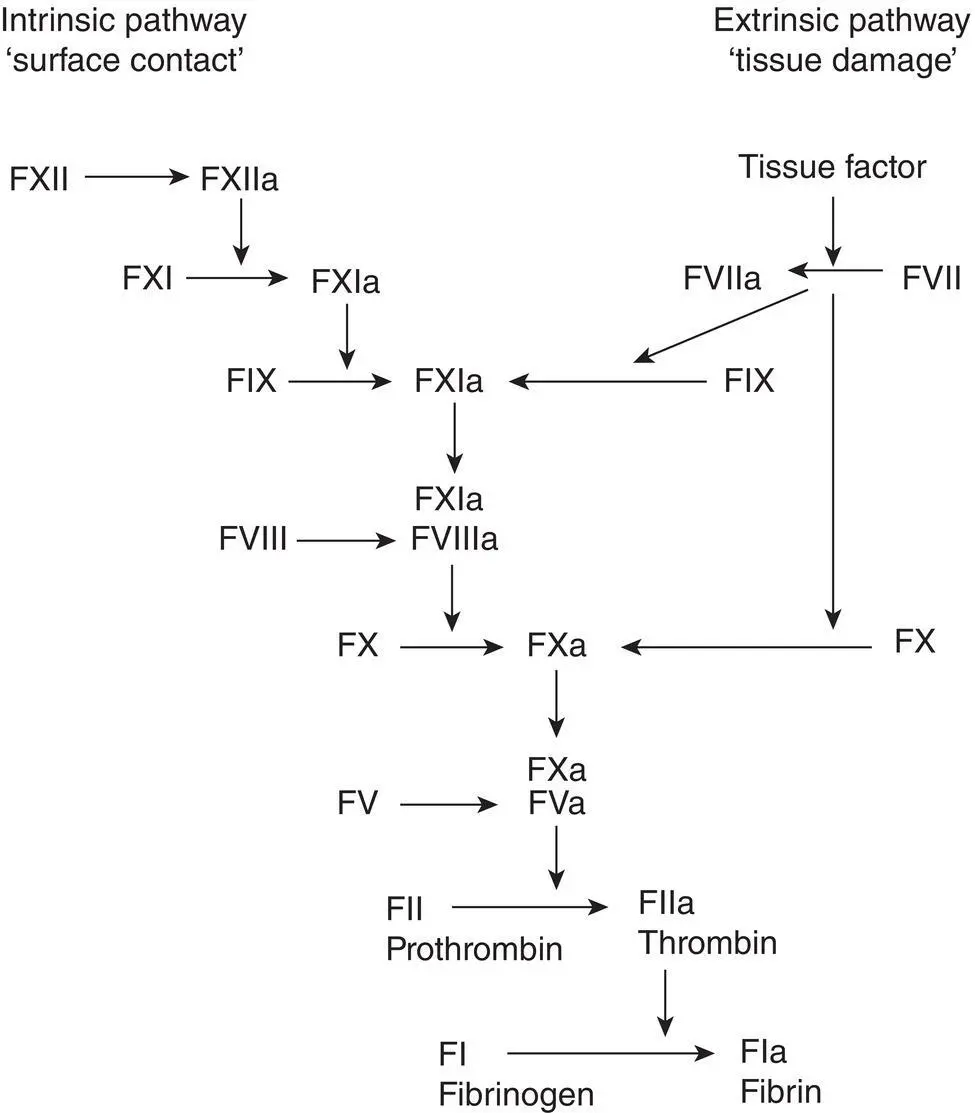
Figure 24.1 Coagulation cascade.
Von Willebrand’s disease is extremely common and has an incidence of up to 1% in the general population. It is autosomally dominantly inherited and, therefore, occurs in males and females equally. The majority of cases are mild; the condition is significantly underdiagnosed, and in milder cases, bleeding occurs only with significant haemostatic challenges. Consequently, mild von Willebrand’s disease can present and be diagnosed at any age. Von Willebrand’s disease is due to a decreased concentration of the protein von Willebrand factor, which is important in mediating platelet adhesion to the subendothelium; von Willebrand factor also circulates non‐covalently bound to coagulation factor VIII and so protects factor VIII from premature proteolytic degradation. Therefore, in von Willebrand’s disease, diminished levels of the von Willebrand factor result in both a mild platelet defect and a mild defect of the coagulation cascade consequent upon the diminished amounts of factor VIII. Unlike in haemophilia, the skin bleeding time is increased, and bleeding tends to be primarily mucocutaneous, with epistaxis, gum bleeding, gastrointestinal bleeding, and menorrhagia. Diagnosis and classification require the determination of factor VIII concentration, the von Willebrand factor antigen, and the von Willebrand factor activity using the ristocetin cofactor activity or collagen‐binding activity and analysis of the von Willebrand factor multimer distribution. Mild type I cases can usually be treated with desmopressin (DDAVP) prior to significant haemostatic challenge, whereas the rarer, more severe forms of von Willebrand’s disease usually require treatment with clotting factor concentrates, which should contain both factor VIII and the von Willebrand factor. 7DDAVP is contraindicated in patients with ischaemic heart disease and uncontrolled hypertension.
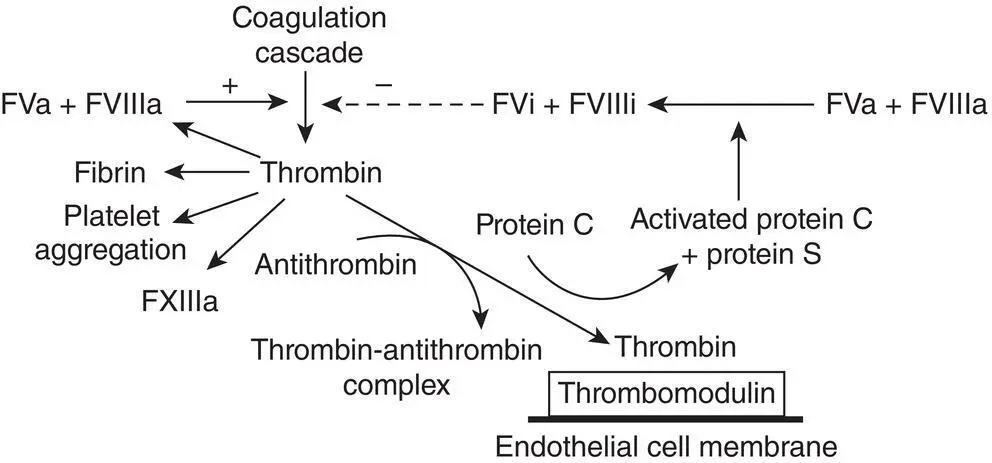
Figure 24.2 The natural anticoagulant pathway directly inhibits and negatively regulates the formation of thrombin by the coagulation cascade.
Table 24.3 Causes of acquired coagulation defects.
| Heparin: unfractionated or low molecular weight |
| Warfarin |
| DOAC: Dabigatran, Rivaroxaban, Apixaban, Edoxaban |
| Liver disease |
| Specific coagulation factor inhibitors |
| Disseminated intravascular coagulation |
| Paraproteins: myeloma, MGUS, amyloid |
Acquired coagulation defects
Probably the most commonly acquired coagulation defect ( Table 24.3) in the elderly is iatrogenic because of the use of the anticoagulants such as unfractionated heparin or low‐molecular‐weight heparin, warfarin, or direct‐acting oral anticoagulants (DOACs). Heparin is given parenterally and acts by potentiating the action of antithrombin to inhibit thrombin. It is a difficult drug to use, with a narrow therapeutic range, complicated pharmacokinetics, and significant interpatient variation in dose requirements. Insufficient heparin will result in thrombosis or extension of previously existing thrombosis, while excess treatment rapidly precipitates haemorrhage, which is potentially life‐threatening. Heparin infusion should be monitored by use of the APTT; the therapeutic range is a ratio of between 1.5 and 2. 8The introduction of low‐molecular‐weight heparins (LMWHs) for both prophylaxis and treatment of venous thrombosis has the significant advantages of a longer half‐life, increased bioavailability, and more predictable pharmacokinetics; consequently, they can be given by once‐daily subcutaneous injection without the need for monitoring, even in the doses required for treatment. Since low‐molecular‐weight heparin has a greater effect on factor Xa than on thrombin (IIa), it cannot be monitored with the APTT but instead requires an antifactor Xa assay. However, in overdosage, even low‐molecular‐weight heparin will prolong the APTT, and bleeding under these circumstances may require neutralization of the heparin with protamine sulfate. 9LMWH use has been shown to have a survival advantage in patients with malignancy and thrombosis and is the anticoagulant of choice in this group.
Читать дальшеИнтервал:
Закладка:
Похожие книги на «Pathy's Principles and Practice of Geriatric Medicine»
Представляем Вашему вниманию похожие книги на «Pathy's Principles and Practice of Geriatric Medicine» списком для выбора. Мы отобрали схожую по названию и смыслу литературу в надежде предоставить читателям больше вариантов отыскать новые, интересные, ещё непрочитанные произведения.








Обсуждение, отзывы о книге «Pathy's Principles and Practice of Geriatric Medicine» и просто собственные мнения читателей. Оставьте ваши комментарии, напишите, что Вы думаете о произведении, его смысле или главных героях. Укажите что конкретно понравилось, а что нет, и почему Вы так считаете.