Pathy's Principles and Practice of Geriatric Medicine
Здесь есть возможность читать онлайн «Pathy's Principles and Practice of Geriatric Medicine» — ознакомительный отрывок электронной книги совершенно бесплатно, а после прочтения отрывка купить полную версию. В некоторых случаях можно слушать аудио, скачать через торрент в формате fb2 и присутствует краткое содержание. Жанр: unrecognised, на английском языке. Описание произведения, (предисловие) а так же отзывы посетителей доступны на портале библиотеки ЛибКат.
- Название:Pathy's Principles and Practice of Geriatric Medicine
- Автор:
- Жанр:
- Год:неизвестен
- ISBN:нет данных
- Рейтинг книги:3 / 5. Голосов: 1
-
Избранное:Добавить в избранное
- Отзывы:
-
Ваша оценка:
Pathy's Principles and Practice of Geriatric Medicine: краткое содержание, описание и аннотация
Предлагаем к чтению аннотацию, описание, краткое содержание или предисловие (зависит от того, что написал сам автор книги «Pathy's Principles and Practice of Geriatric Medicine»). Если вы не нашли необходимую информацию о книге — напишите в комментариях, мы постараемся отыскать её.
Pathy’s Principles and Practice of Geriatric Medicine
Pathy's Principles and Practice of Geriatric Medicine — читать онлайн ознакомительный отрывок
Ниже представлен текст книги, разбитый по страницам. Система сохранения места последней прочитанной страницы, позволяет с удобством читать онлайн бесплатно книгу «Pathy's Principles and Practice of Geriatric Medicine», без необходимости каждый раз заново искать на чём Вы остановились. Поставьте закладку, и сможете в любой момент перейти на страницу, на которой закончили чтение.
Интервал:
Закладка:
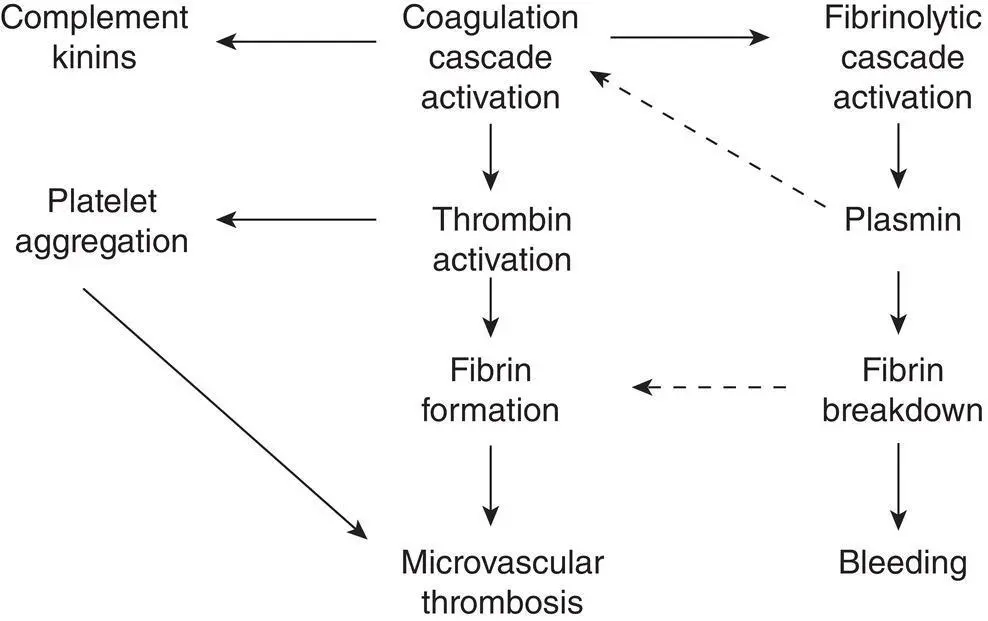
Figure 23.1 Mechanism of microvascular thrombosis and bleeding in DIC. Broken lines indicate inhibition.
Table 23.1 Mechanisms and precipitating factors in DIC.
| Mechanism | Example |
|---|---|
| Coagulation cascade activation | Tissue factor exposure in trauma and extensive surgery |
| Fibrinolytic cascade activation | Plasminogen activators liberated in acute promyelocytic leukaemia or disseminated prostatic cancer |
| Intravascular platelet aggregation | Haemolytic uraemic syndrome, thrombotic thrombocytopenic purpura, heparin‐induced thrombocytopenia |
| Endothelial cell activation | Gram‐negative sepsis, disseminated malignancy |
| Direct proteolytic cleavage of haemostatic proteins | Pancreatitis, snake venoms |
The bleeding in DIC is multifactorial in origin as a result of depletion of fibrinogen, all coagulation factors, and platelets as a consequence of consumption due to uncontrolled and excessive activation of the coagulation cascade, diminished platelet number due to consumption, and an additional or acquired platelet defect consequent to proteolytic degradation of platelet surface glycoproteins and partial degranulation of α and dense platelet granules. Hyperfibrinolysis leads to elevated levels of fibrinogen and fibrin degradation products (measured as highly increased D‐dimers), which act as competitive inhibitors of fibrin polymerization. The uncontrolled generation of free thrombin and plasmin degrades fibrin, fibrinogen, and coagulation factors, particularly factors V and VIII. Consequently, there is a systemic bleeding diathesis resulting in not only bleeding from local surgical incisions or traumatic wounds but also generalized bruising, petechiae, and purpura, together with bleeding from sites of venepuncture, arterial lines, drains, catheters, and endotracheal tubes. There is also frequent gastrointestinal bleeding, haemoptysis, haematuria, and even intramuscular or intracerebral bleeding. Clinically, the widespread occurrence of abnormal and excessive bleeding is the hallmark of DIC. Excessive bleeding from a single site, particularly following surgery, is usually more indicative of a specific failure of local haemostasis than DIC and requires specific local measures. The microvascular thrombosis results in anoxic damage and ischaemic infarction of vital organs, including lungs, kidneys, brain, pituitary, liver, adrenal, heart, and skin. 6
Diagnosis
The diagnosis of DIC is made in the presence of a predisposing cause, the clinical manifestations of systemic bleeding and multiorgan dysfunction, and appropriate laboratory investigations ( Table 23.2). The haemoglobin is usually reduced owing to intravascular red cell fragmentation, resulting in a microangiopathic haemolytic anaemia (MAHA), and there is profound thrombocytopenia. Coagulation times are abnormal, with a prolongation of the activated partial thromboplastin time (APTT), prothrombin time (PT), and thrombin time (TT) and depletion of fibrinogen, all due to consumption. In addition, there is evidence of fibrinolytic activation and fibrin degradation with elevations of serum FDPs or plasma D‐dimers. As well as these rapid and readily available tests, recent studies have shown that waveform analysis of the coagulation profile on automated machines can have both diagnostic and prognostic significance, and laboratory abnormalities can be included in a validated scoring system for DIC. In addition to consumption of the coagulation factors and prolongation of the clotting times, levels of natural anticoagulant pathway proteins – antithrombin, protein C, and protein S – are also significantly reduced, contributing to microvascular thrombosis. 7
Table 23.2 Laboratory diagnosis of DIC.
| Test | Result |
|---|---|
| APTT | Prolonged >10 seconds beyond normal |
| PT | Prolonged > 5 seconds beyond normal |
| TT | Prolonged > 10 seconds beyond normal |
| Fibrinogen | Low, usually <1 g l −1 |
| Platelets | Low, usually <50 × 10 9l −1 |
| D‐dimer | Raised > 1000 ng/ml |
As DIC is a dynamic condition, it is preferable to perform the simple clotting tests frequently, both before and after clinical interventions, to judge their efficacy and the need for further blood product replacement therapy or interventions. The role of thromboelastography (TEG) in monitoring DIC has progressed in recent years, with the use of whole blood and near‐patient testing, particularly in operating theatres, able to direct the appropriate component to replace when bleeding is excessive.
Management
The first principle of managing DIC should be toward resuscitation of the patient to achieve adequate oxygenation, blood pressure, circulation, and renal perfusion. Once resuscitation is complete, aggressive treatment of the DIC's underlying precipitating cause should be addressed. Most frequently, this is sepsis, and aggressive broad‐spectrum antibiotic therapy is necessary following the taking of appropriate microbiological samples. A few causes of disseminated malignancy, such as acute promyelocytic leukaemia and hormone‐responsive breast and prostatic carcinoma, may also be amenable to treatment, but the prognosis in DIC secondary to disseminated malignancy is usually poor; indeed, mortality overall remains high at 25–75% in various series.
There is considerable controversy about the place of blood product support in DIC. Clearly, red cells and platelet support, together with plasma product support, are indicated in actively bleeding patients. In patients who are not actively bleeding or requiring surgical or other intervention, the use of transfused clotting factors and platelets only makes the microvascular thrombosis worse unless the underlying precipitating factors have been treated. However, once these issues have been addressed, if the patient is bleeding, it is appropriate to transfuse red cells to achieve a haemoglobin level of above 10 g l −1or haematocrit above 30%, to transfuse platelets to achieve a platelet count of >80 × 10 9l −1, to transfuse FFP (10–15 ml kg −1) to correct the PT and APTT to no more than 10% prolonged above the upper limit of normal, and to increase the fibrinogen to >1 g l −1through the appropriate use of cryoprecipitate (cryoprecipitate is particularly rich in fibrinogen) or fibrinogen concentrate. Following blood product intervention, the clotting screen should be repeated to assess the response to therapy and the need for additional future therapy.
In DIC due to sepsis, there is now evidence that depletion of the natural anticoagulant pathway proteins such as antithrombin, protein C, and protein S contributes to microvascular thrombosis, the systemic inflammatory response, and a poorer prognosis. It is not clear if replacement of natural anticoagulants is of therapeutic benefit, but several trials have been published, especially with antithrombin concentrate, with inconclusive results.
The use of heparin is even more controversial. 8,9There are no adequate controlled trials to support its use, and although it would appear logical to use an anticoagulant in a condition where the major morbidity and mortality are due to thrombosis, the use of a systemic anticoagulant in patients either with active bleeding or at high risk of catastrophic bleeding is problematic. Furthermore, there are considerable problems in determining the dose and duration of treatment and monitoring heparin therapy in the presence of severely prolonged clotting times. As heparin works by potentiating the activity of antithrombin, which is usually severely depleted in DIC, its efficacy is uncertain. Fibrinolytic therapy with tranexamic acid is contraindicated in DIC unless the trigger mechanism is hyperfibrinolysis, and the use of aprotinin, prostacyclin, and antiplatelet drugs remains controversial and unproven. There is evidence that human recombinant activated FVIIa may be useful in uncontrolled life‐threatening haemorrhage, but it should be recognized that the product is not licensed for this indication; and its use in systemic bleeding disorders outside of haemophilia and platelet disorders is associated with a significant increase in arterial thrombotic events, particularly heart attacks and cerebrovascular accidents.
Читать дальшеИнтервал:
Закладка:
Похожие книги на «Pathy's Principles and Practice of Geriatric Medicine»
Представляем Вашему вниманию похожие книги на «Pathy's Principles and Practice of Geriatric Medicine» списком для выбора. Мы отобрали схожую по названию и смыслу литературу в надежде предоставить читателям больше вариантов отыскать новые, интересные, ещё непрочитанные произведения.








Обсуждение, отзывы о книге «Pathy's Principles and Practice of Geriatric Medicine» и просто собственные мнения читателей. Оставьте ваши комментарии, напишите, что Вы думаете о произведении, его смысле или главных героях. Укажите что конкретно понравилось, а что нет, и почему Вы так считаете.