Successful Training in Gastrointestinal Endoscopy
Здесь есть возможность читать онлайн «Successful Training in Gastrointestinal Endoscopy» — ознакомительный отрывок электронной книги совершенно бесплатно, а после прочтения отрывка купить полную версию. В некоторых случаях можно слушать аудио, скачать через торрент в формате fb2 и присутствует краткое содержание. Жанр: unrecognised, на английском языке. Описание произведения, (предисловие) а так же отзывы посетителей доступны на портале библиотеки ЛибКат.
- Название:Successful Training in Gastrointestinal Endoscopy
- Автор:
- Жанр:
- Год:неизвестен
- ISBN:нет данных
- Рейтинг книги:3 / 5. Голосов: 1
-
Избранное:Добавить в избранное
- Отзывы:
-
Ваша оценка:
Successful Training in Gastrointestinal Endoscopy: краткое содержание, описание и аннотация
Предлагаем к чтению аннотацию, описание, краткое содержание или предисловие (зависит от того, что написал сам автор книги «Successful Training in Gastrointestinal Endoscopy»). Если вы не нашли необходимую информацию о книге — напишите в комментариях, мы постараемся отыскать её.
Teaches trainee gastroenterologists the endoscopic skills needed to meet the medical training requirements to practice gastroenterology and helps clinical specialists refresh their skills to pass their recertification Successful Training in Gastrointestinal Endoscopy, Second Edition
Successful Training in Gastrointestinal Endoscopy, Second Edition
Successful Training in Gastrointestinal Endoscopy — читать онлайн ознакомительный отрывок
Ниже представлен текст книги, разбитый по страницам. Система сохранения места последней прочитанной страницы, позволяет с удобством читать онлайн бесплатно книгу «Successful Training in Gastrointestinal Endoscopy», без необходимости каждый раз заново искать на чём Вы остановились. Поставьте закладку, и сможете в любой момент перейти на страницу, на которой закончили чтение.
Интервал:
Закладка:
Evolution and types of endoscopy simulators
Static models
The initial attempts to complement endoscope training with simulators utilized static models. Such “phantoms” were intended to teach basic hand–eye coordination, the use of the endoscope dials, and even the recognition of basic pathology. In the 1970s, as upper endoscopy and colonoscopy were becoming established as important modalities, other models were developed. These included the Heinkel hemispheric anatomical model [18] and the upper GI plastic dummy introduced by Classen [19].
In the early 1970s, homemade demonstration models of the colon, featuring a mobile transverse colon and the ability to demonstrate an “N” or alpha loop, were devised ( Figure 1.2). In 1972, a colonoscopy model fashioned from the spiral metal‐reinforced tubing of a hair dryer was introduced, with the ability to demonstrate corkscrewing movements ( Figure 1.3). This early simulator featured the ability for the colonoscope to “become stuck” and then to be “straightened out.” Christopher Williams’ St. Marks/KeyMed colonoscopy model of 1975, shown in Figure 1.4, had an improved feeling of realism and was made commercially available. Twisting movements were required to negotiate the lumen, and endoscopists found it challenging [20].

Figure 1.2 Roller demonstration model (1971): Homemade model showing alpha loop and mobile transverse colon.
(Courtesy: Dr. Christopher Williams.)
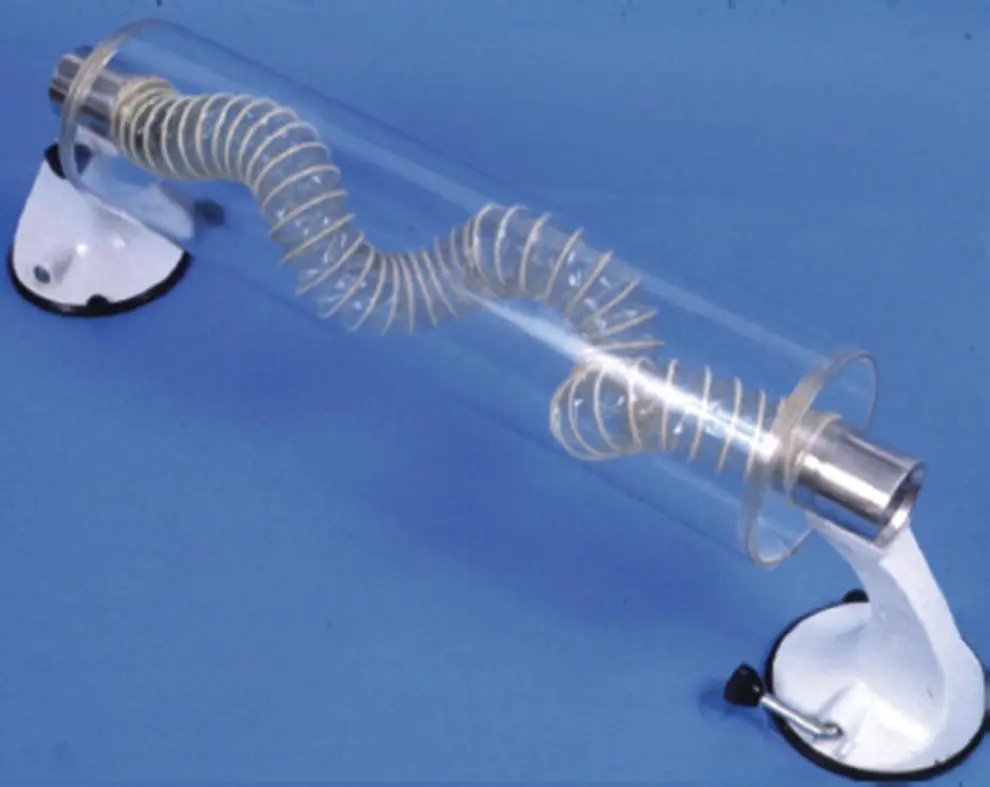
Figure 1.3 Hair dryer tube model (1972).
(Courtesy: Dr. Christopher Williams.)
Simultaneously, hand–eye coordination models were developed. These included an electronic targeting model ( Figure 1.5), which had a photocell at the center, tested two‐handed coordination, and allowed for “scoring” of results. An endoscopic version of the popular game “Pong” was even developed in 1977 ( Figure 1.6), allowing for reinforcement of left/right coordination maneuvers in an enjoyable and motivating “game.”

Figure 1.4 St Mark’s/KeyMed model (1975): Commercially available with semirealistic feel.
(Courtesy: Dr. Christopher Williams.)

Figure 1.5 Electronic targeting model (1975): Tested hand–eye coordination.
(Courtesy: Dr. Christopher Williams.)
The Imperial College/St Mark’s College Simulator was introduced in 1980 ( Figure 1.7) and allowed for insertion of a limited amount of the shaft of an endoscope into the computer model, with real‐time video feedback. This model demonstrated that such devices were feasible, although the particular model was limited by the fragility of the microswitches. Improvements were made over the ensuing 5 years, and by 1985, an updated and substantially more robust version of that simulator existed. The MK2 simulator allowed full “shaft” insertion, a sensation of resistance during looping, and audio tracks to simulate patient “complaints” ( Figure 1.8). The computer allowed for a database and record keeping. Still, the simulator was felt to be crude and somewhat unrealistic.

Figure 1.6 Endoscopic Pong Game (1977): Tested hand–eye coordination.
(Courtesy: Dr. Christopher Williams.)
In 1992, Leung and Chung developed a static model and described its use in teaching ERCP [21]. Unfortunately, the utility of each of these models has been limited by their inability to truly simulate realistic conditions. To date, while these static learning devices can be useful in instruction and learning of appropriate manipulation of the endoscope within the bowel lumen, they offer little in the way of simulated pathology. The lack of motility, the “feel” of actual compliant tissue, and the inability to practice therapeutic maneuvers have largely limited the use of static models to introductory training.
Perhaps, the most comprehensive application of static models in endoscopic teaching was described by Lucero et al. in 1995 [22]. This group designed a psychomotor training program called SimPrac‐EDF y VEE (simulator for the practice of fiberoptic digestive endoscopy and electronic video endoscopy). Moreover, they described a series of courses in which they included static models and superimposed painted pictures to recreate frequently seen endoscopic abnormalities. These courses featured didactic lessons, slides, tapes, and supervised hands‐on training on models. In addition to the Lucero model, those of Classen and Heinkel were also used. A specific Billroth II model was designed to demonstrate the unique features of this altered anatomy. Participants were offered sessions with increasingly challenging manual and cognitive tasks; faculty at the course assessed objective skills of the participants [22].
In Lucero’s courses, 8–25 individuals were included in each particular workshop, and trainees had a mean duration of hands‐on practice of 28 hours. In all, 422 trainees in over 22 such courses were described, and the authors noted that 95% of trainees demonstrated an “acceptable level of skill” by the end of the training [22]. However, the authors failed to describe other details of the possible benefits of such training. Such courses would appear to be difficult logistically to conduct and hugely labor intensive. Perhaps, the most important contribution of this work was the concept of integrating various hands‐on training tools into a comprehensive training program that combined didactic lesions, cognitive training, and specific hands‐on exercise geared to develop particular skill sets. Lucero’s use of a patterned lesson plan integrated into multimodality workshops using expert faculty, a blend of manual training and cognitive skills, and immediate feedback and evaluation served as a model for subsequent efforts using more realistic and sophisticated simulators. As such, it remains an important example for future endeavors in endoscopic training.
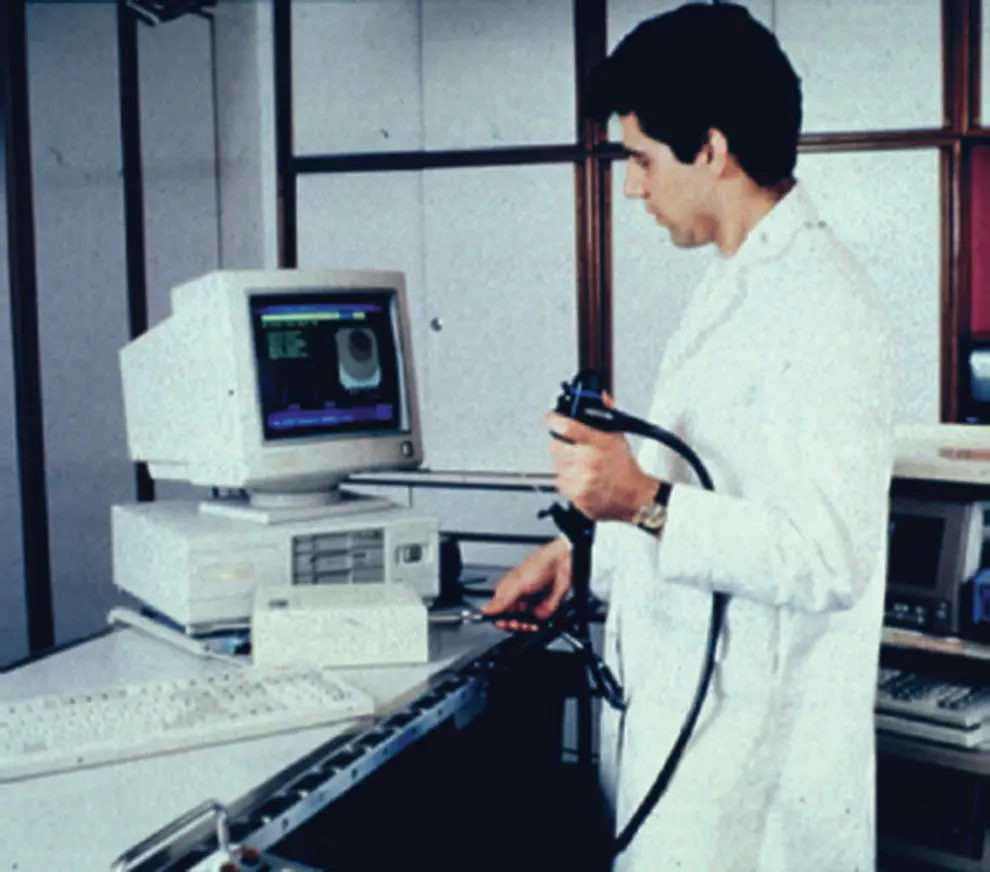
Figure 1.7 Imperial College/St Mark’s simulator (1980): Limited shaft insertion, but feasibility of simulator demonstrated.
(Courtesy: Dr. Christopher Williams.)

Figure 1.8 Imperial College/St Mark’s simulator MK2 (1985): Full shaft insertion and audible “complaints.”
(Courtesy: Dr. Christopher Williams.)
Since that time, static models evolved in two distinct directions. Two ERCP static trainers were designed that allow for complex therapeutic procedure performance and team training between endoscopist and assistant. These are described in detail in Chapter 8( Figure 1.9a,b).
Читать дальшеИнтервал:
Закладка:
Похожие книги на «Successful Training in Gastrointestinal Endoscopy»
Представляем Вашему вниманию похожие книги на «Successful Training in Gastrointestinal Endoscopy» списком для выбора. Мы отобрали схожую по названию и смыслу литературу в надежде предоставить читателям больше вариантов отыскать новые, интересные, ещё непрочитанные произведения.










Обсуждение, отзывы о книге «Successful Training in Gastrointestinal Endoscopy» и просто собственные мнения читателей. Оставьте ваши комментарии, напишите, что Вы думаете о произведении, его смысле или главных героях. Укажите что конкретно понравилось, а что нет, и почему Вы так считаете.