Brenda A. Wilson - Bacterial Pathogenesis
Здесь есть возможность читать онлайн «Brenda A. Wilson - Bacterial Pathogenesis» — ознакомительный отрывок электронной книги совершенно бесплатно, а после прочтения отрывка купить полную версию. В некоторых случаях можно слушать аудио, скачать через торрент в формате fb2 и присутствует краткое содержание. Жанр: unrecognised, на английском языке. Описание произведения, (предисловие) а так же отзывы посетителей доступны на портале библиотеки ЛибКат.
- Название:Bacterial Pathogenesis
- Автор:
- Жанр:
- Год:неизвестен
- ISBN:нет данных
- Рейтинг книги:5 / 5. Голосов: 1
-
Избранное:Добавить в избранное
- Отзывы:
-
Ваша оценка:
Bacterial Pathogenesis: краткое содержание, описание и аннотация
Предлагаем к чтению аннотацию, описание, краткое содержание или предисловие (зависит от того, что написал сам автор книги «Bacterial Pathogenesis»). Если вы не нашли необходимую информацию о книге — напишите в комментариях, мы постараемся отыскать её.
Completely revised and updated, and for the first time in stunning full-color, Bacterial Pathogenesis: A Molecular Approach, Fourth Edition, builds on the core principles and foundations of its predecessors while expanding into new concepts, key findings, and cutting-edge research, including new developments in the areas of the microbiome and CRISPR as well as the growing challenges of antimicrobial resistance. All-new detailed illustrations help students clearly understand important concepts and mechanisms of the complex interplay between bacterial pathogens and their hosts. Study questions at the end of each chapter challenge students to delve more deeply into the topics covered, and hone their skills in reading, interpreting, and analyzing data, as well as devising their own experiments. A detailed glossary defines and expands on key terms highlighted throughout the book. Written for advanced undergraduate, graduate, and professional students in microbiology, bacteriology, and pathogenesis, this text is a must-have for anyone looking for a greater understanding of virulence mechanisms across the breadth of bacterial pathogens.
Bacterial Pathogenesis — читать онлайн ознакомительный отрывок
Ниже представлен текст книги, разбитый по страницам. Система сохранения места последней прочитанной страницы, позволяет с удобством читать онлайн бесплатно книгу «Bacterial Pathogenesis», без необходимости каждый раз заново искать на чём Вы остановились. Поставьте закладку, и сможете в любой момент перейти на страницу, на которой закончили чтение.
Интервал:
Закладка:
Questions
1. How does a DNA-based analysis, such as the 16S rRNA gene analysis, differ from a cultivation-based analysis? In this chapter, the DNA-based approaches have been emphasized. What are some advantages of the cultivation-based approach?
2. More and more research groups are seeking to show that changes in the microbiota of a particular site are involved in diseases such as periodontal disease, inflammatory bowel disease, and premature birth. Critics object that showing an association is not the same as demonstrating cause and effect. In the case of the obesity study, scientists tried to do this by inoculating germfree mice with different variations of the microbiota. Clearly, this would not be possible in humans. How might you prove cause and effect in humans?
3. Infants in the first years of life are often more susceptible to certain bacterial infections than older children. How can you explain this? What function of the microbiota does this illustrate?
4. Members of the microbiota cause some quite serious diseases. How could a bacterium that normally lives in a beneficial or neutral association with its human host cause serious disease?
5. Metabolic interactions between members of the microbiota are attracting more attention because two microbes working together can increase the effectiveness of a reaction catalyzed by one of them. Consider an association between a polysaccharide-fermenting microbe and a methanogen in the colon. Consider also that the overall energy of a reaction depends on the ratio of substrate to end products for a bacterium like a polysaccharide fermenter. Can you explain why a polysaccharide fermenter and a methanogen might team up in the colon?
6. The assertion is made in this chapter that scientists now believe that transfer of DNA by conjugation in the colon is occurring across species and genus lines. Suppose you found the same type of antibiotic-resistance gene in members of two different genera. What criteria might you use to show that the gene was transferred horizontally? How might you suspect that the gene was transferred by conjugation?
7. Conventional wisdom asserts that there are no methanogens in the vaginal tract. If they were present they would probably be present at low levels. How would you use the 16S rRNA approach to find them? What modification of the approach used to find bacterial sequences would you have to make?
8. PCR combined with sequencing can provide a quick identification of bacteria. What are the limitations of this approach?
9. Resident microbiotas provide protection from colonization of some pathogenic bacteria in certain parts of the body. Describe regions of the body where normal microbiotas are protective and how they accomplish this protection.
For each of the following, choose the most correct answer:
10. The “normal” microbiota of humans is
a. constantly changing.
b. commensal.
c. the same in every individual.
d. parasitic.
11. Removing most of the microorganisms from the intestinal tract would
a. inhibit infections.
b. have no effect on health.
c. lead to diarrhea and maybe other diseases.
d. improve digestion.
12. Which of the following statements about normal microbiotas is not true?
a. Our bodies begin to acquire a normal microbiota within a week of birth.
b. Microbial communities, once established, remain constant throughout one’s lifetime.
c. At the cellular level, our bodies are approximately 50% bacteria.
d. Normal microbiotas can cause disease in humans.
13. Clostridium difficile is an example of
a. how antibiotic use can cause a disease by disturbing the gut microbiota.
b. how a shift in the bacterial microbiota of the gums can cause disease.
c. how a shift in the eukaryotic microbiota of the vaginal tract can cause disease.
d. a bacterium that is capable of surviving in the human stomach.
e. a bacterium that is normally carried in the human nose.
14. Helicobacter pylori is
a. a major component of the microbiota of the human small intestine.
b. a cause of ulcers in the human stomach.
c. responsible for most of the lactic acid production in the stomach.
d. allows yeast to overgrow after antibiotic treatment.
e. associated with gum disease and bad breath when a microbiota shift occurs.
15. The reservoir hypothesis refers to the
a. effect of antibiotics on the composition of the oral microbiota.
b. transfer of genes among bacteria in the human colon.
c. shifts in bacterial populations that are associated with diet.
d. differences in the prokaryotic-to-eukaryotic ratio.
e. presence of Gram-positive bacteria in the vaginal tract.
16. A normal microbiota in the duodenum is
a. similar to the microbiota in the stomach.
b. similar to the microbiota in the colon.
c. tolerant to acidic environments.
d. both A and C.
e. both B and C.
17. In the absence of the full complement of the normal microbiota, due to orally taken antibiotics, opportunistic microorganisms such as _______ can become established and cause disease.
a. Clostridium difficile
b. Proteus mirabilis
c. Staphylococcus aureus
d. all of the above
e. none of the above
Solving Problems in Bacterial Pathogenesis
1. You are a researcher working for the U.S. Department of Agriculture. After two years of effort, you have isolated in pure culture a new, highly virulent bacterium from duck feces that is responsible for several major outbreaks of deaths in mammalian wildlife from contaminated pond water in the South. Based on 16S rRNA sequence comparison, you have determined that this new bacterium is distantly related to the Gram-negative bacterium Vibrio cholerae, and you have named the new strain Vibrio birdsii. You find that ducks are apparently unaffected by V. birdsii. You suspect that V. birdsii may be part of the normal microbiota of ducks. To test this hypothesis, you set up an experiment to examine the host response to V. birdsii in germfree ducks. The results are summarized in the graph shown in Figure 1. Provide a detailed explanation and interpretation for the results. Do the results support the hypothesis? Provide a rationale for your answer.
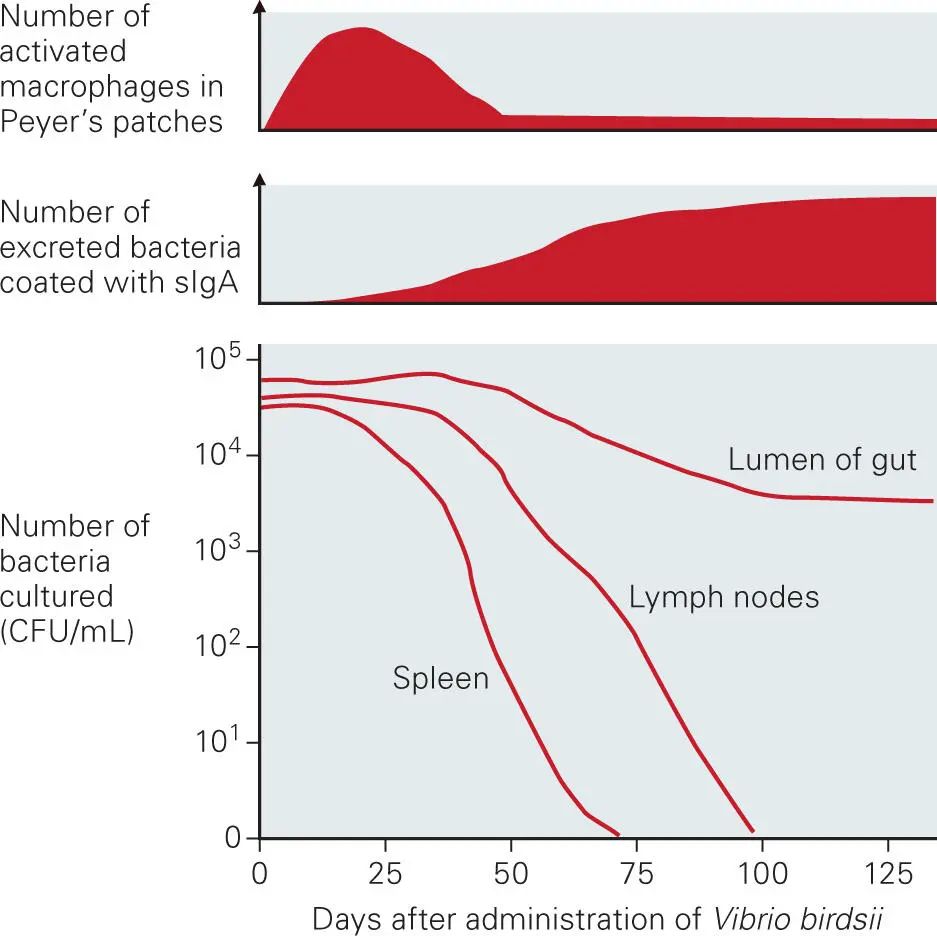
Figure 1. Results.
2. Dental plaque is a biofilm consisting of a complex community of over 700 different bacterial species. Epidemiological evidence suggests that a population shift toward certain Gram-negative anaerobes is responsible for initiation and progression of periodontal diseases. Tannerella forsythia, a Gram-negative, filamentous, nonmotile, anaerobic bacterium, is also considered one of the pathogens implicated in contributing to advanced forms of periodontal disease in humans and is strongly associated with cases of severe periodontitis. It is found co-aggregated in periodontal pockets with other putative periodontal pathogens, such as Porphyromonas gingivalis and Fusobacterium nucleatum. Infection with T. forsythia induces alveolar bone resorption in a mouse infection model, in which the bacterium is inoculated under the gums of mice, followed by measuring for loss of dental bone. Considering that periodontal disease might be a community shift-type disease with multiple microbial participants, how might you use microbial community profiling methods to demonstrate the importance of the microbial community composition in contributing to the onset and maintenance of the diseased state? Set up the experiment first without using DNA sequencing approaches and then with using DNA sequencing approaches. Be sure to provide your rationale for method choice. From your results, how could you distinguish between a model of disease caused by a microbial community shift involving multiple microbes and one involving a single pathogen, such as T. forsythia or P. gingivalis, or a combination of both T. forsythia and P. gingivalis?
Читать дальшеИнтервал:
Закладка:
Похожие книги на «Bacterial Pathogenesis»
Представляем Вашему вниманию похожие книги на «Bacterial Pathogenesis» списком для выбора. Мы отобрали схожую по названию и смыслу литературу в надежде предоставить читателям больше вариантов отыскать новые, интересные, ещё непрочитанные произведения.




Обсуждение, отзывы о книге «Bacterial Pathogenesis» и просто собственные мнения читателей. Оставьте ваши комментарии, напишите, что Вы думаете о произведении, его смысле или главных героях. Укажите что конкретно понравилось, а что нет, и почему Вы так считаете.