Lynne Shore Garcia - Diagnostic Medical Parasitology
Здесь есть возможность читать онлайн «Lynne Shore Garcia - Diagnostic Medical Parasitology» — ознакомительный отрывок электронной книги совершенно бесплатно, а после прочтения отрывка купить полную версию. В некоторых случаях можно слушать аудио, скачать через торрент в формате fb2 и присутствует краткое содержание. Жанр: unrecognised, на английском языке. Описание произведения, (предисловие) а так же отзывы посетителей доступны на портале библиотеки ЛибКат.
- Название:Diagnostic Medical Parasitology
- Автор:
- Жанр:
- Год:неизвестен
- ISBN:нет данных
- Рейтинг книги:3 / 5. Голосов: 1
-
Избранное:Добавить в избранное
- Отзывы:
-
Ваша оценка:
Diagnostic Medical Parasitology: краткое содержание, описание и аннотация
Предлагаем к чтению аннотацию, описание, краткое содержание или предисловие (зависит от того, что написал сам автор книги «Diagnostic Medical Parasitology»). Если вы не нашли необходимую информацию о книге — напишите в комментариях, мы постараемся отыскать её.
Diagnostic Medical Parasitology — читать онлайн ознакомительный отрывок
Ниже представлен текст книги, разбитый по страницам. Система сохранения места последней прочитанной страницы, позволяет с удобством читать онлайн бесплатно книгу «Diagnostic Medical Parasitology», без необходимости каждый раз заново искать на чём Вы остановились. Поставьте закладку, и сможете в любой момент перейти на страницу, на которой закончили чтение.
Интервал:
Закладка:
When considering available options and laboratory test menus, it is important to make sure that the pros and cons of the approaches selected are thoroughly understood and that diagnostic tests, potential results, and reporting formats are carefully explained to all clients. As an example, if the results of a stool examination are based on a concentration sediment examination only, this information must be conveyed to the physician. Many of the intestinal protozoa are missed by this diagnostic test approach, and it is important for the physician to recognize the limitations of such testing. Most physicians receive very little, if any, exposure to medical parasitology in medical school, and many newer physicians trained as generalists or family practitioners also have limited parasitology training or experience.
In most cases, it is probably realistic to assume that patients are symptomatic if they are submitting stool specimens for diagnostic parasitology testing. In an excellent article by Hiatt et al., the premise tested was that a single stool sample from a symptomatic patient would be sufficient to diagnose infections with intestinal protozoa ( 23). However, with additional stool examinations for symptomatic patients, the yield of intestinal protozoa increased dramatically (Entamoeba histolytica, 22.7% increase; Giardia lamblia, 11.3% increase; and Dientamoeba fragilis, 31.1% increase). This publication again demonstrates the problems with performing only a single stool examination (using the ova and parasite examination). If the patient becomes asymptomatic after the first stool examination, it may be acceptable to discontinue the series of stool examinations (this should be a clinician decision).
Available options are compared to the “gold standard,” which includes a series of three stool examinations (direct, concentrate, and permanent stained smear for a fresh specimen; concentrate and permanent stained smear for a preserved specimen). The single-specimen pros and cons are discussed in the previous paragraph (symptomatic versus asymptomatic patients). A suggestion has been made to pool three specimens and to perform a single concentration and a single permanent stained smear. Depending on the number of positives and negatives, this may be a viable option, but some organisms may be missed. Another testing option for three pooled specimens might be to perform a single concentration and three separate permanent stained smears. This approach would probably increase the yield of intestinal protozoa over the previous option. Another suggestion involves placing a sample of each of three stools into a single vial of preservative. This collection approach would require only a single vial, but it is very likely that the vial would be overfilled and that mixing and the ratio of fixative to stool would be inaccurate.
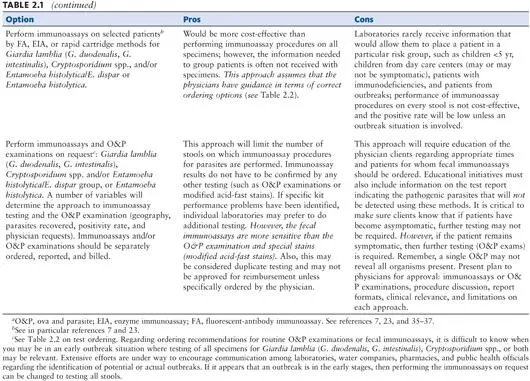
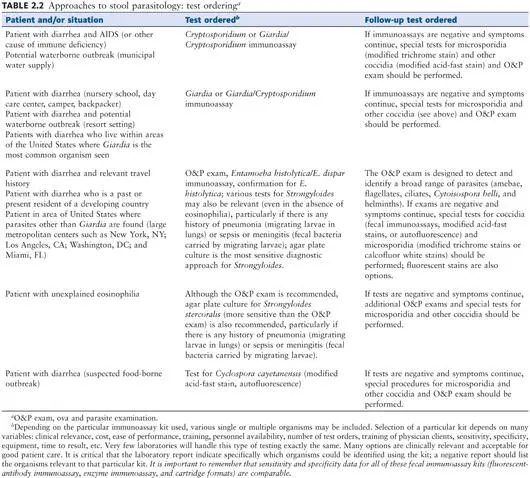
One could also test patient specimens by using immunoassay reagents or kits for Giardia lamblia (G. duodenalis, G. intestinalis), the Entamoeba histolytica/E. dispar group, Entamoeba histolytica, or Cryptosporidium spp. However, patient history information is rarely received with the clinical specimen; fecal testing based on patient risk group or situation is impossible without sufficient information. Testing of patient specimens by immunoassay procedures should be performed on request; however, client education is critical for successful implementation of this approach. Collection and testing options and the pros and cons of each are listed in Tables 2.1and 2.2.

The Clinical and Laboratory Standards Institute (formerly the National Committee for Clinical Laboratory Standards) document Procedures for the Recovery and Identification of Parasites from the Intestinal Tract (Approved Guideline M28-2A) was updated in 2005. Various stool collection, processing, and testing options are also included in that publication ( 1, 25).
In summary, laboratories performing diagnostic parasitology testing must decide on the appropriate test methods that are relevant for their own operations based on a number of variables mentioned above. It is unrealistic to assume or state that one approach is applicable for every laboratory; however, it is important to thoroughly understand the options within your test menu and to convey this information to your clients once your approach has been selected for implementation. Prior discussion with clients, written educational memos, meetings, and examples of revised report formats are highly recommended prior to implementation.
Collection Times
A series of three specimens as indicated above should be submitted on separate days; if possible, the specimens should be submitted every other day; otherwise, the series of three specimens should be submitted within no more than 10 days. If a series of six specimens is requested, the specimens should also be collected on separate days or within no more than 14 days. Many organisms, particularly the intestinal protozoa, do not appear in the stool in consistent numbers on a daily basis, and the series of three specimens is considered a minimum for an adequate examination. It is inappropriate for multiple specimens to be submitted from the same patient on the same day. One possible exception would be stool collections from a patient who has severe, watery diarrhea such that any organisms present might be missed because of the tremendous dilution factor related to fluid loss. Even under these circumstances, acceptance of more than one specimen per patient per day should not be routine but should be done only after consultation with the physician. It is also not recommended for the three specimens to be submitted one each day for three consecutive days; however, use of this collection time frame would not be sufficient cause to reject the specimens. Adequate spacing between specimens helps to provide parasite recovery within the recommended time frames.
Although the recommended number of stool specimens is three, laboratories have been more willing to accept two specimens, primarily because of cost savings and the assumption that if the patient is symptomatic, confirmation of any organisms present is just as likely to be possible from two specimens as from three specimens. However, it is important that clients understand the pros and cons of two compared with three stools. Both collection approaches are being used by diagnostic laboratories.
Specimen Type, Specimen Stability, and Need for Preservation
Fresh specimens are mandatory for the recovery of motile trophozoites (amebae, flagellates, or ciliates). The protozoan trophozoite stage is normally found in cases of diarrhea; the gastrointestinal tract contents are moving through the system too rapidly for cyst formation to occur. Once the stool specimen is passed from the body, trophozoites do not encyst but may disintegrate if not examined or preserved within a short time after passage. The time limit recommendations listed below are most relevant for the intestinal protozoa; most helminth eggs and larvae, coccidian oocysts, and microsporidian spores survive for extended periods. However, no one can predict which organisms will be present in the stool specimens; therefore, it is important to use the most conservative time frames for parasite recovery.
Liquid specimens should be examined within 30 min of passage, not 30 min from the time they reach the laboratory. If this general time recommendation of 30 min is not possible, the specimen should be placed in one of the available fixatives. Soft (semiformed) specimens may contain a mixture of protozoan trophozoites and cysts and should be examined within 1 h of passage; again, if this time frame is not possible, preservatives should be used. Immediate examination of formed specimens is not as critical; in fact, if the specimen is examined at any time within 24 h after passage, the protozoan cysts should still be intact ( 5, 16).
Читать дальшеИнтервал:
Закладка:
Похожие книги на «Diagnostic Medical Parasitology»
Представляем Вашему вниманию похожие книги на «Diagnostic Medical Parasitology» списком для выбора. Мы отобрали схожую по названию и смыслу литературу в надежде предоставить читателям больше вариантов отыскать новые, интересные, ещё непрочитанные произведения.




Обсуждение, отзывы о книге «Diagnostic Medical Parasitology» и просто собственные мнения читателей. Оставьте ваши комментарии, напишите, что Вы думаете о произведении, его смысле или главных героях. Укажите что конкретно понравилось, а что нет, и почему Вы так считаете.