Hannie van Genderen - Schema Therapy for Borderline Personality Disorder
Здесь есть возможность читать онлайн «Hannie van Genderen - Schema Therapy for Borderline Personality Disorder» — ознакомительный отрывок электронной книги совершенно бесплатно, а после прочтения отрывка купить полную версию. В некоторых случаях можно слушать аудио, скачать через торрент в формате fb2 и присутствует краткое содержание. Жанр: unrecognised, на английском языке. Описание произведения, (предисловие) а так же отзывы посетителей доступны на портале библиотеки ЛибКат.
- Название:Schema Therapy for Borderline Personality Disorder
- Автор:
- Жанр:
- Год:неизвестен
- ISBN:нет данных
- Рейтинг книги:3 / 5. Голосов: 1
-
Избранное:Добавить в избранное
- Отзывы:
-
Ваша оценка:
Schema Therapy for Borderline Personality Disorder: краткое содержание, описание и аннотация
Предлагаем к чтению аннотацию, описание, краткое содержание или предисловие (зависит от того, что написал сам автор книги «Schema Therapy for Borderline Personality Disorder»). Если вы не нашли необходимую информацию о книге — напишите в комментариях, мы постараемся отыскать её.
Shema Therapy for Borderline Personality Disorder
Schema Therapy for Borderline Personality Disorder
Schema Therapy for Borderline Personality Disorder — читать онлайн ознакомительный отрывок
Ниже представлен текст книги, разбитый по страницам. Система сохранения места последней прочитанной страницы, позволяет с удобством читать онлайн бесплатно книгу «Schema Therapy for Borderline Personality Disorder», без необходимости каждый раз заново искать на чём Вы остановились. Поставьте закладку, и сможете в любой момент перейти на страницу, на которой закончили чтение.
Интервал:
Закладка:
The therapist is very attentive to the way the patient treats him. From the behavior of the patient he can gather information about the schemas, modes and the coping strategies of the patient.
The process of treating a BPD patient seldom begins with a calm conversation of information collection and case conceptualization. One should not be surprised when this process of information gathering is more of a rollercoaster as opposed to a quiet drive in the country. Often from day one it is clear that the patient is not comfortable or in a state to embark on a constructive relationship with the therapist. The development of a therapeutic relationship and the gathering of information will be discussed in the next chapter.
Experiential techniques
The patient's personal history is mapped and put into relation with the emergence of the schema modes. The therapist analyses which experiences in the past have contributed to the current problems. This is often not easy to find out in a more cognitive way. Here, it is recommended to use a short imagery exercise to examine the link between the past and the present (see Chapter 5) or a two chair technique (see Chapter 6).
We recommend using imagery at least one or two times in the phase of case conceptualization. In this way the patient can discover links between her present problems and her schema modes or between her past and her schema modes (See ST step by step 1.03) If the patient is unable to imagine unpleasant events from the past, the therapist can also suggest an imagery with her father and/or mother. The instruction is that it doesn't have to be an uncomfortable situation but can be a neutral or typical situation. Usually this imagery can also give relevant information for the case conceptualization.
Case conceptualization
Together the therapist and patient create a case conceptualization based upon the mode model (see Chapter 2). The different modes are described to the patient in terms she can understand and identify with (see Figure 3.1). They link the different modes with relevant experiences from the past and current complaints (see ST step by step 1.04 and 1.05)
It is recommended to link the relevant schemas to each mode in order to understand which schemas are triggered when a mode is active. Especially when the abandoned/ abused child is triggered it is relevant to know that in patient X the mistrust/abuse schema is most prominent and in patient Y defectiveness/shame is the central issue. This gives the therapist extra information about the content of the limited reparenting.
It is important that the most important problems and BPD‐traits of the patient can be understood as manifestations of the modes. There is no one‐to‐one relationship of specific BPD symptoms to modes. The therapist and the patient should collaborate in finding out what the function of the symptom is, before the symptom can be linked to a mode. For instance, self‐injury or a suicide attempt can have different functions, for example:
to punish oneself for a certain behavior or for having an emotional need (then it is a manifestation of the punitive parent mode)
to distract from emotional pain (then it is a manifestation of the detached protector mode)
to signal despair and alarm others that they should take care of the patient—a cry for help (then it is manifestation of the abandoned/abused child mode)
to make others feel guilty about how they treated the patient—as an act of revenge (then it is a manifestation of the angry child mode).
Even in the same patient, the same symptom may have different functions, depending on the triggers and the context, and should therefore be linked to different modes. Apart from symptoms and other problems having a function, symptoms and problems can also be consequences. For example, a low mood may be the consequence of being so often in the detached protector mode that there are too few positive experiences in the patient's life, in which case the low mood should be connected to the detached protector mode.
BPD patients usually have many problems and symptoms, therefore the therapist should not strive for completeness. It suffices to place the most important problems and symptoms in the mode model, keeping the problems that the patient experiences as most debilitating in mind.
The therapist creates a mode model together with Nora, with names for the modes that best suit the patient's experience, ( Figure 3.1). They gradually expand this model with the relevant schemas and the elements from her childhood that are the cause of the problems ( Figure 3.2).
Explaining the treatment rationale
Once a diagnosis of BPD has been established, the therapist begins to explain the rationale behind the therapy by means of the BPD model and its modes (see ST step by step 1.06). He explains how the patient's current problems are connected to schemas and modes. He further explains how each schema mode brings along with its certain feelings, thoughts, and behaviors (see Appendix A: ST for patients). For a more in‐depth explanation, the patient can refer to a number of relevant chapters in Breaking Negative Thinking Patterns (Jacob, van Genderen, & Seebauer, 2015) or Reinventing Your Life (Young & Klosko, 1994).
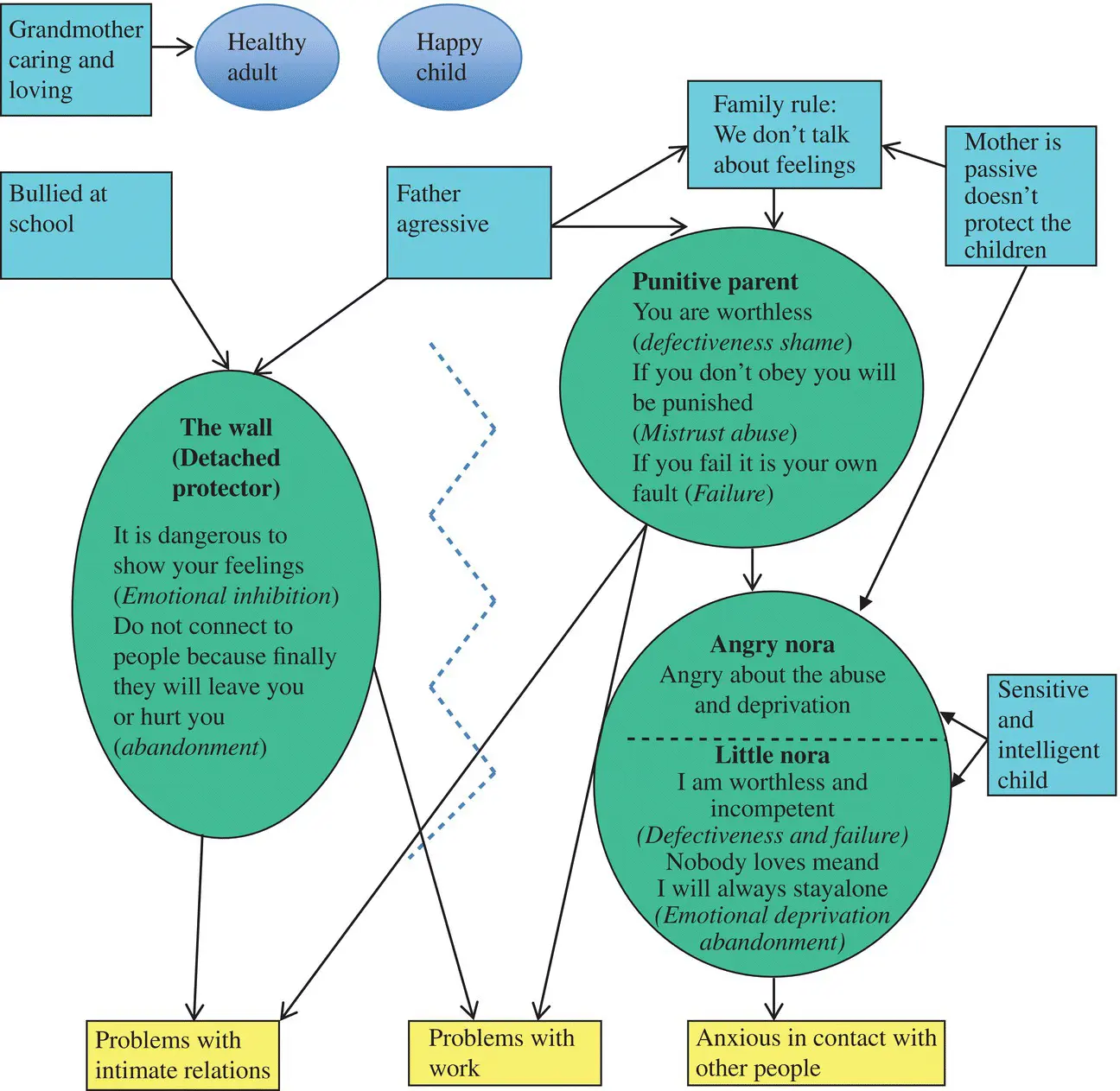
Figure 3.2 Mode model with schemas and historical roots Nora
Most BPD patients find the experience of learning about the borderline model enlightening. It offers a clear explanation as to why they experience sudden mood swings and have so little control over their behavior (see Chapter 9, “A Simultaneous Chess Play in a Pinball Machine”). It also offers them the hope that change is possible and that they are not doomed to a life filled with uncontrolled behavior and mood swings.
If the patient finds that this model is not appropriate to her situation, there are usually three possibilities: one is that the individual simply does not have BPD. The second one is that important modes are overlooked, in which case these have to be added to the patient's mode conceptualization. The last possibility is that despite the person having BPD, there is also a very strong protector mode at work. Because of this protector, everything the therapist says is considered to be dubious and unreliable. A variant of this is when the patient recognizes parts of the model, but denies other parts, for example, the punitive parent mode, as acknowledging that mode is yet too frightening. If the latter is the case, the therapist must take more time in building a trusting relationship with the patient and not dwell upon attempting to convince the patient of the schema model.
Crisis management
Crisis management can be skipped when there is no crisis present at the beginning of the therapy. However, for BPD patients it is recommended to make a crisis management plan together with the patient and to relate this to the modes. Different modes can be active in different crises and might need different actions.
The (short‐term) risks of a crisis should be discussed with the patient. The actual handling of a crisis is returned to later in the therapy in case it occurs. Should a crisis be present, it indeed requires the highest attention (see Chapter 8, “Crisis”).
Treatment phase: therapeutic interventions with schema modes
This is the central phase of therapy and has a duration of about a year (see Chapters 5– 10). The general goals of this stage are
Learn to recognize when one of the modes is active
Читать дальшеИнтервал:
Закладка:
Похожие книги на «Schema Therapy for Borderline Personality Disorder»
Представляем Вашему вниманию похожие книги на «Schema Therapy for Borderline Personality Disorder» списком для выбора. Мы отобрали схожую по названию и смыслу литературу в надежде предоставить читателям больше вариантов отыскать новые, интересные, ещё непрочитанные произведения.





Обсуждение, отзывы о книге «Schema Therapy for Borderline Personality Disorder» и просто собственные мнения читателей. Оставьте ваши комментарии, напишите, что Вы думаете о произведении, его смысле или главных героях. Укажите что конкретно понравилось, а что нет, и почему Вы так считаете.