Clinical Pancreatology for Practising Gastroenterologists and Surgeons
Здесь есть возможность читать онлайн «Clinical Pancreatology for Practising Gastroenterologists and Surgeons» — ознакомительный отрывок электронной книги совершенно бесплатно, а после прочтения отрывка купить полную версию. В некоторых случаях можно слушать аудио, скачать через торрент в формате fb2 и присутствует краткое содержание. Жанр: unrecognised, на английском языке. Описание произведения, (предисловие) а так же отзывы посетителей доступны на портале библиотеки ЛибКат.

- Название:Clinical Pancreatology for Practising Gastroenterologists and Surgeons
- Автор:
- Жанр:
- Год:неизвестен
- ISBN:нет данных
- Рейтинг книги:4 / 5. Голосов: 1
-
Избранное:Добавить в избранное
- Отзывы:
-
Ваша оценка:
Clinical Pancreatology for Practising Gastroenterologists and Surgeons: краткое содержание, описание и аннотация
Предлагаем к чтению аннотацию, описание, краткое содержание или предисловие (зависит от того, что написал сам автор книги «Clinical Pancreatology for Practising Gastroenterologists and Surgeons»). Если вы не нашли необходимую информацию о книге — напишите в комментариях, мы постараемся отыскать её.
was first published sixteen years ago, the knowledge and clinical management of pancreatic diseases have developed markedly. Thanks to the development of translational research and the “from bench to bedside” concept, much progress from the lab has been applied to clinical practice. Additionally, several highly relevant clinical trials published over the last decade have resulted in the updating and optimisation of clinical guidelines.
A new and validated classification of the severity and complications of acute pancreatitis that is firmly rooted in clinical practice has become the basis for the development of minimally invasive approaches to pancreatic necrosis. The etiopathogenic knowledge of chronic pancreatitis and other pancreatopaties, like that associated with diabetes mellitus, has developed significantly. Increased study of cystic pancreatic tumours, which has been reflected in the publication of several guidelines and consensus reports over the last few years, is especially important. Most research efforts have focused on pancreatic cancer, which have led and will further lead to a significant increase in the therapeutic armamentarium against this devastating disease. Finally, many newly published studies have changed the concept, causes, clinical relevance, diagnosis and treatment of exocrine pancreatic insufficiency. Updates based on these developments and more are included in the new edition of
.
This new edition of
is a result of the collaboration between the world's leading experts in each area of clinical pancreatology, with the aim of facilitating gastroenterologists, surgeons, oncologists, internists, nutritionists, diabetologists, paediatricians, radiologists, pathologists and other specialists in their daily clinical practice. This book is an indispensable update providing leading knowledge in clinical pancreatology.
Clinical Pancreatology for Practising Gastroenterologists and Surgeons — читать онлайн ознакомительный отрывок
Ниже представлен текст книги, разбитый по страницам. Система сохранения места последней прочитанной страницы, позволяет с удобством читать онлайн бесплатно книгу «Clinical Pancreatology for Practising Gastroenterologists and Surgeons», без необходимости каждый раз заново искать на чём Вы остановились. Поставьте закладку, и сможете в любой момент перейти на страницу, на которой закончили чтение.
Интервал:
Закладка:
Necrotizing Pancreatitis
Acute necrotizing pancreatitis occurs in about 10% of patients with acute pancreatitis, and is associated with a considerably higher mortality and morbidity than in those who have IEP. Pancreatic necrosis refers to nonviable parenchyma, and can be focal or diffuse. The Revised Atlanta Classification system has divided pancreatic necrosis into three subtypes based on anatomic location: pancreatic parenchyma, peripancreatic fat, and both pancreatic parenchyma and peripancreatic fat. Early diagnosis of pancreatic necrosis can be done using either post‐contrast CT or MRI examination [8]. Necrotizing pancreatitis is clinically diagnosed when more than 30% of the gland is affected by necrosis [9].
Parenchymal necrosis is seen as well‐demarcated low signal areas on T1‐weighted pre‐contrast sequences corresponding to nonenhancing areas on post‐contrast sequences [10]. However, evaluation of pancreatic necrosis is less accurate during the first week after the onset of acute pancreatitis. In the most acute phase of pancreatitis, increased parenchymal edema may result in decreased enhancement of viable pancreatic tissue, which limits the reliable estimation of necrosis. After a week or more, resolution of this acute parenchymal edema will improve the enhancement of any viable tissue, leaving truly nonviable tissue able to be more accurately diagnosed and quantified.
MRI is also useful in the detection of hemorrhage, as MRI is highly sensitive to the paramagnetic effect of the methemoglobin that is deposited in the setting of bleeding. Hemorrhage is recognized on MRI as high signal intensities on fat‐suppressed T1‐ and T2‐weighted images. Conversely, chronic hematoma can be hypointense on both T1‐ and T2‐weighted images due to transformation of methemoglobin into hemosiderin [11].
Table 6.1 MRI protocol for evaluating acute or chronic pancreatitis.
| MRI sequence | Target organ | MRI findings |
|---|---|---|
| T1‐weighted gradient echo 2D or 3D. Dixon, nonfat suppressed, axial, breath‐hold. Axial slice thickness 6 mm | Parenchyma | Pancreatic inflammation: low signal |
| T2‐weighted single‐shot fast spin echo. 2D, nonfat suppressed, axial and coronal, breath‐hold. Axial and coronal slice thickness 4 mm | Pancreatic and biliary ducts. | Pancreatic inflammation: increased signal Fluid collection and cystic lesions: high signal intensity Ductal stones, abnormal side branches |
| T2‐weighted turbo spin echo 2D. Fat‐suppressed respiratory or navigator triggered. Axial slice thickness 6 mm | Parenchyma and retroperitoneum | Parenchymal and peripancreatic fat inflammation: increased signal |
| T2‐weighted 3D MRCP respiratory or navigator triggered high resolution. Coronal 40‐mm 3D slab | Ductal evaluation | 3D MRCP provides ERCP‐like high‐resolution duct images. Disconnected duct, fistula, abnormal side branches, ductal anomalies; pancreas divisum |
| T2‐weighted 2D MRCP, breath‐hold, coronal 40 mm single shot | Ductal evaluation and secretin enhancement | Pancreatic abnormalities, disconnected or disrupted duct, pancreas exocrine capacity |
| T1‐weighted gradient echo 3D, fat suppressed, breath‐hold. Axial, 2‐mm reconstruction | Parenchymal organs and vessels | Pancreatic inflammation: decreased enhancement Pancreatic necrosis: no enhancement Vessels, active hemorrhage, pseudoaneurysm |
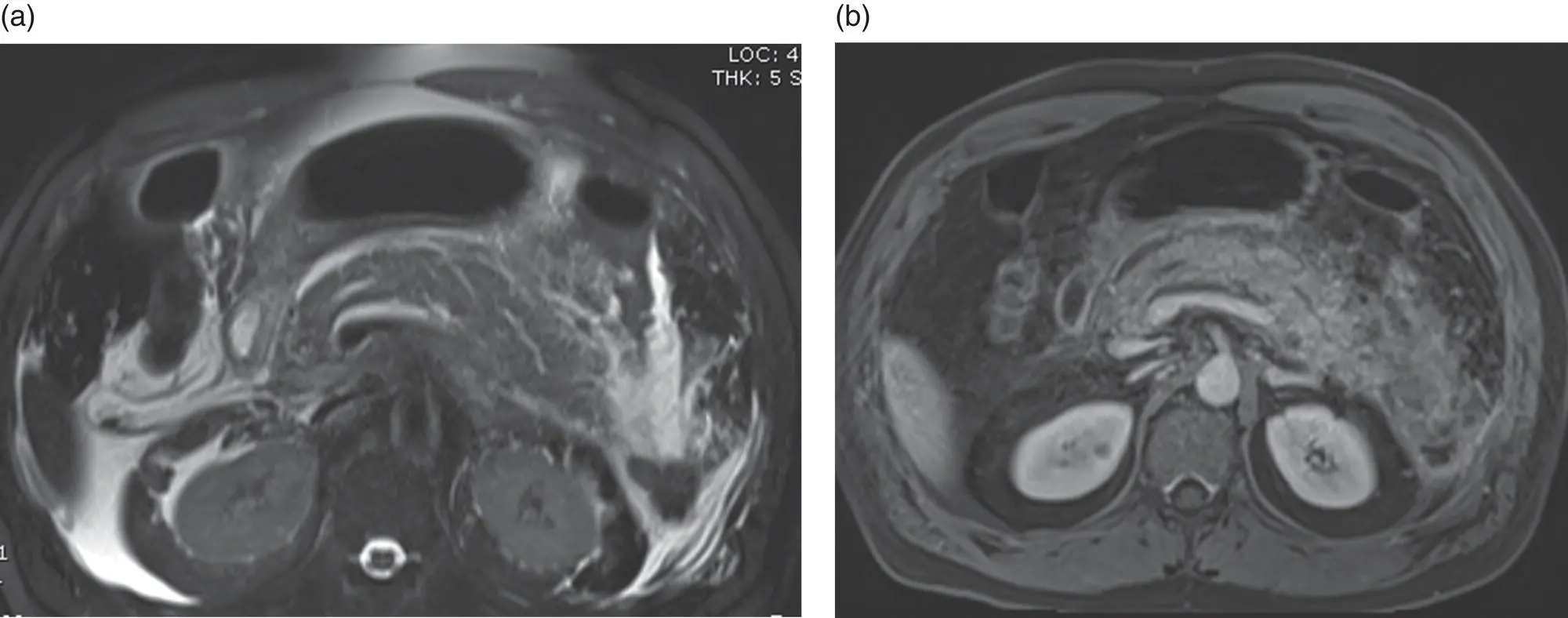
Figure 6.1 A 44‐year‐old male presents with acute onset of severe abdominal pain and elevated lipase. (a) Axial T2‐weighted fat‐suppressed image demonstrates acute pancreatitis with hyperintense peripancreatic fluid and pancreatic parenchyma due to interstitial edema. (b) Post‐contrast T1‐weighted image demonstrates decreased enhancement of parenchyma.
Sources: (a) courtesy of Fatih Akisik; (b) Sandrasegaran et al. [7]. Reproduced with permission of American Journal of Roentgenology .
Pancreatic necrosis is responsible for approximately 40% of cases of disconnected pancreatic duct. In the presence of residual functioning pancreatic parenchyma upstream to the disconnected pancreatic duct, fluid collections or peripancreatic ascites will develop. T2‐weighted MRCP images will show a disconnected pancreatic duct often connected to adjacent fluid collection. In some cases, the pancreatic duct may not be completely disconnected but a focal rupture can cause leakage and/or fistula formation. In both entities, enlarging fluid collection(s) may be seen. Retrospective analysis of cases of pancreatic duct disruption show that MRCP identified significantly more cases than ERCP (91% vs. 74%) [12].
Complications of Acute Pancreatitis
Fluid Collections
The Atlanta classification system has standardized the terminology used to discuss the fluid collections commonly associated with acute pancreatitis.
Acute Peripancreatic Fluid Collection
Acute peripancreatic fluid collection (APFC) is an early complication of acute IEP and does not exhibit any discernible walls. This fluid is amylase and lipase rich, and develops within the first 48 hours in 30–50% of patients with acute pancreatitis. The majority of cases resolve spontaneously within two to four weeks [13]. MRI will show low signal areas on T1‐weighted and high signal areas on T2‐weighted images.
Acute Necrotic Collection
Acute necrotic collection (ANC) contains both liquefied and nonliquefied necrotic material. Early in the course of pancreatitis, both APFC and ANC have similar imaging findings, but the presence of pancreatic necrosis allows the diagnosis of ANC. Diagnosis of ANC can be more reliable a week after onset of pancreatitis, as peripancreatic fat necrosis is more likely to develop. MRI of ANC shows heterogeneous low signal on T1‐weighted and heterogeneous high signal on T2‐weighted images. Hemorrhage is not uncommon with pancreatic necrosis and will be seen as areas of high signal on T1‐weighted images. The presence of an actively bleeding vessel can be depicted on post‐contrast dynamic imaging as a contrast blush or as gradually increasing signal in the collection.
Pseudocyst
Pseudocyst occurs after four weeks from unresolved APFC, as the fluid becomes more organized. On MRI, this appears as an organized T2‐weighted hyperintense fluid collection, and may demonstrate a thin surrounding rim on post‐contrast images. It should be noted that the presence of even a small area of internal fat or soft‐tissue attenuation within the fluid collection should not be seen with a pseudocyst; the presence of these changes the designation of the fluid collection to walled‐off necrosis. Pseudocysts may connect to the pancreatic ductal system, which can be seen with MRCP images. Secretin‐enhanced MRCP significantly improves visualization of such connections.
Walled‐off Necrosis
Walled‐off necrosis, similar to pseudocyst formation, develops after four weeks, but from an ANC as opposed to an APFC. It has a thick mature wall and contains necrotic fat and/or pancreatic tissues and fluid. On T2‐weighted images, different than pseudocyst, nonliquefied debris is present in the collection ( Figure 6.2a). Post‐contrast T1‐weighted images will show an enhancing wall ( Figure 6.2c).
MRI is highly accurate and reliable in making the diagnosis of any of these fluid collections, and in evaluating for possible connections with the pancreatic ductal system ( Figure 6.2b) [14].
Читать дальшеИнтервал:
Закладка:
Похожие книги на «Clinical Pancreatology for Practising Gastroenterologists and Surgeons»
Представляем Вашему вниманию похожие книги на «Clinical Pancreatology for Practising Gastroenterologists and Surgeons» списком для выбора. Мы отобрали схожую по названию и смыслу литературу в надежде предоставить читателям больше вариантов отыскать новые, интересные, ещё непрочитанные произведения.












Обсуждение, отзывы о книге «Clinical Pancreatology for Practising Gastroenterologists and Surgeons» и просто собственные мнения читателей. Оставьте ваши комментарии, напишите, что Вы думаете о произведении, его смысле или главных героях. Укажите что конкретно понравилось, а что нет, и почему Вы так считаете.