The Veterinary Dental Patient - A Multidisciplinary Approach
Здесь есть возможность читать онлайн «The Veterinary Dental Patient - A Multidisciplinary Approach» — ознакомительный отрывок электронной книги совершенно бесплатно, а после прочтения отрывка купить полную версию. В некоторых случаях можно слушать аудио, скачать через торрент в формате fb2 и присутствует краткое содержание. Жанр: unrecognised, на английском языке. Описание произведения, (предисловие) а так же отзывы посетителей доступны на портале библиотеки ЛибКат.
- Название:The Veterinary Dental Patient: A Multidisciplinary Approach
- Автор:
- Жанр:
- Год:неизвестен
- ISBN:нет данных
- Рейтинг книги:3 / 5. Голосов: 1
-
Избранное:Добавить в избранное
- Отзывы:
-
Ваша оценка:
The Veterinary Dental Patient: A Multidisciplinary Approach: краткое содержание, описание и аннотация
Предлагаем к чтению аннотацию, описание, краткое содержание или предисловие (зависит от того, что написал сам автор книги «The Veterinary Dental Patient: A Multidisciplinary Approach»). Если вы не нашли необходимую информацию о книге — напишите в комментариях, мы постараемся отыскать её.
The Veterinary Dental Patient: A Multidisciplinary Approach
The Veterinary Dental Patient: A Multidisciplinary Approach — читать онлайн ознакомительный отрывок
Ниже представлен текст книги, разбитый по страницам. Система сохранения места последней прочитанной страницы, позволяет с удобством читать онлайн бесплатно книгу «The Veterinary Dental Patient: A Multidisciplinary Approach», без необходимости каждый раз заново искать на чём Вы остановились. Поставьте закладку, и сможете в любой момент перейти на страницу, на которой закончили чтение.
Интервал:
Закладка:
Figure 5.1 Dental Index app.
5.3 Established Regular Oral Home Care
5.3.1 Importance of Home Dental Care
Home care is an essential component of effective periodontal therapy. Bacterial plaque forms on tooth surfaces within 24 hours of cleaning (Boyce et al. 1995; Wiggs and Lobprise 1997) and will begin to calcify into calculus within one day (Tibbitts and Kashiwa 1998) ( Figure 5.2). Without regular home care, therefore, gingival infection and inflammation quickly recurs (within two weeks) (Payne et al. 1975; Corba et al. 1986a,b; Fiorellini et al. 2006; Rober 2007; Debowes 2010). A human study found that professional cleanings were of little value without home care (Needleman et al. 2005).
In cases of established periodontal disease, home care is even more important. A human study found that periodontal pockets become reinfected within two weeks of a prophylaxis and that pocket depth returns to pretreatment depths within six weeks of therapy if home care is not performed (Rober 2007).
5.3.2 Client Discussion/Instruction
The benefits of routine home care should be conveyed to each client on a regular basis. Homecare should ideally be discussed on their first visitto the practice, which is often the well puppy/kitten or vaccination visit (Wiggs and Lobprise 1997) ( Figure 5.2). Early institution of dental home care provides the greatest benefit, as the frequency of care can be lessened if it is started before periodontal disease (even gingivitis) begins (Tromp et al. 1986a,b). More importantly, early institution of home care increases acceptance by the patient and makes training easier. The importance of home care should also be discussed following each dental cleaning. Compliance may be increased by providing detailed instructions and demonstrations. Ideally, such instruction should be offered and respected by the entire staff (Wiggs and Lobprise 1997).
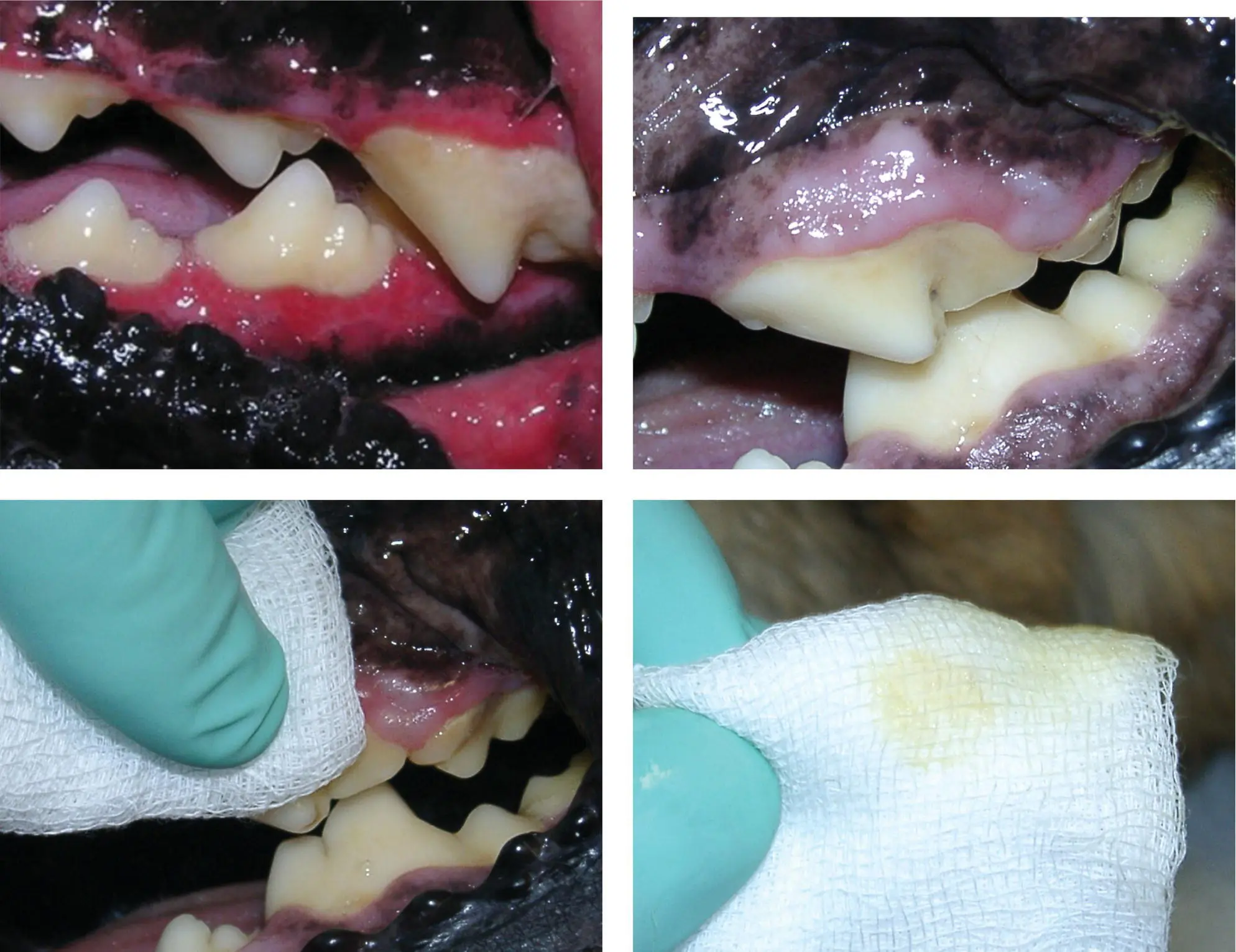
Figure 5.2 Dental plaque identification is part of pet owner education, and should be discussed ideally on the first visit to the practice.
5.3.3 Goals of Home Plaque Control
The primary goal of home plaque control is to limit or reduce the amount of plaque on the teeth (Perry 2006). This in turn should decrease the level of gingival inflammation and, ultimately, of periodontal disease. However, it will not eliminate the need for professional cleanings (Hale 2003).
It is important to note that supragingival plaque and calculus has little to no effect on periodontal disease. It is the plaque at and below the gingival margin that creates inflammation and initiates periodontal disease (Harvey and Emily 1993; Westfelt et al. 1998; Niemiec 2008). Therefore, controlling marginal and subgingival plaque is the key to maintaining periodontal health. Keep this in mind when reviewing various home care options. Information on the suitability of different methods of plaque control is covered later.
Brushing is the most effective means of mechanically removing plaque (Hale 2003). Chew‐based products may be effective, but only if properly formulated. However, oral sprays, rinses, and water additives are in this authors opinion an insufficient means of plaque control, due to the tenacity with which plaque adheres to the teeth and the high resistance of the plaque biofilm to antiseptics (reported to be up to 500 000 times that of singular bacteria: Williams 1995; Quirynen et al. 2006).
5.3.4 Types of Home Care
There are two major types of home plaque control: active and passive. Both can be effective if performed correctly and consistently, but active home care is the “gold standard” (Hale 2003). Typical methods of active home care are brushing and rinsing. Passive methods are typically based on chewing behaviors via treats or specially formulated diets, though recently water additives have been introduced. It has been shown that active home care is most effective on the rostral teeth (incisors and canines) while passive home care is more effective on the distal teeth (premolars and molars) (Bjone et al. 2007; Capik 2007).
5.3.4.1 Active Home Care
Active home care is defined as the client actively participating in the removal of plaque. This can be achieved either by brushing or by rinsing/applying antiseptic/antiplaque solutions.
5.3.4.1.1 Tooth Brushing
When properly performed, tooth brushing is the most effective means of plaque control (Hale 2003). Therefore, while compliance is rare, all veterinarians should still promote tooth brushing for all patients.
5.3.4.1.2 Materials and Methods
The only critical piece of equipment is a toothbrush. There are numerous veterinary brushes available, 1 which should be selected based on patient size. Double‐ and triple‐sided 2 , 3 and circular feline brushes 4 are effective products and should be considered along with the standard veterinary brushes ( Figure 5.3). This author does not recommend “finger brushes” as they do not generally address the subgingival areas of the teeth; additionally, they significantly increase the chances of the owner being bitten. Gauzes and washcloths are not recommended for the same reasons (Holmstrom et al. 1998).
Human toothbrushes may be substituted, with soft‐bristled brushes typically being recommended. A child's toothbrush is often the correct size for small patients and may be more effective than the larger veterinary version. An infant brush may work best for toy‐breed dogs, cats, or juvenile patients.

Figure 5.3 Double‐headed toothbrushes have certain benefits in plaque control.
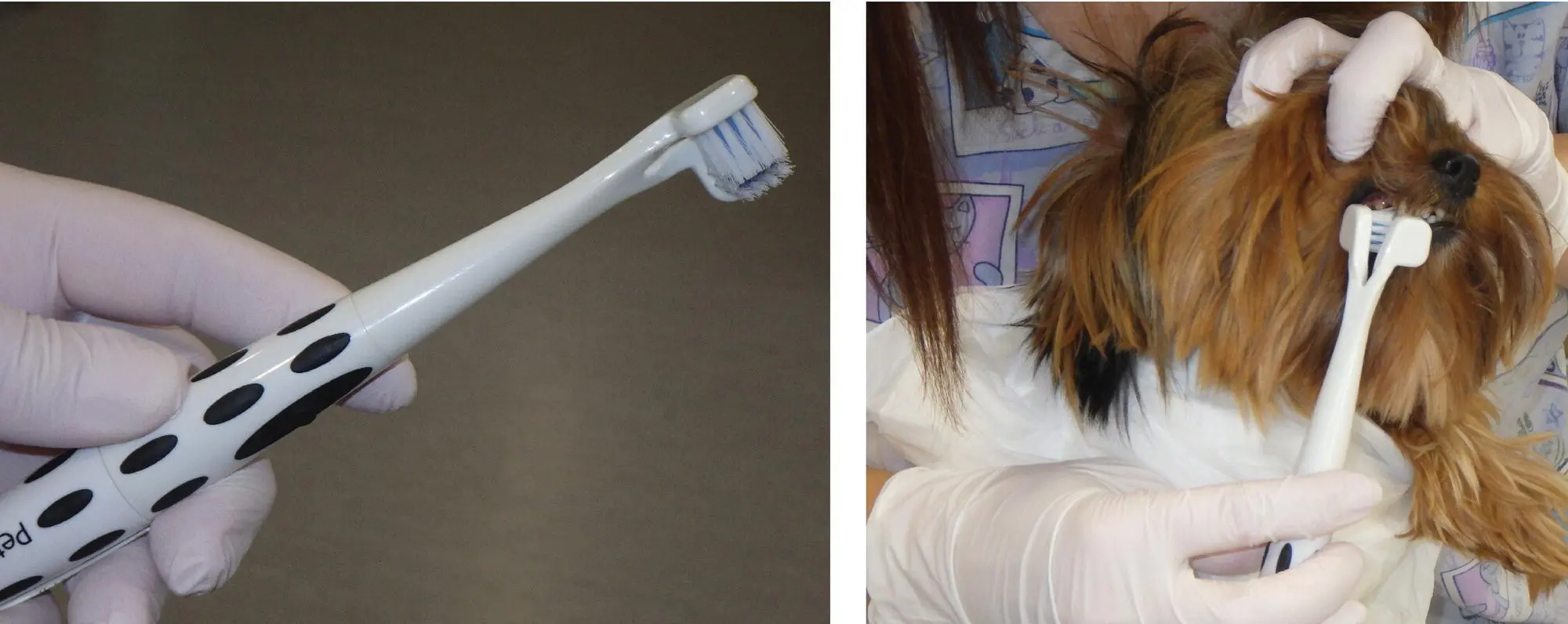
Figure 5.4 Mechanized toothbrush used in dogs.
Mechanized (sonic 5 and rotary 6 ) brushes are superior to standard brushes for humans (Deery et al. 2004; Moritis et al. 2008) ( Figure 5.4). These products are also likely superior for use in veterinary patients, and may make the process more time efficient, which is important in animal patients for acceptance reasons. In addition to the numerous human product options, there is currently a mechanized veterinary brush on the market. 7 One concern with these brushes is that the movement/vibration can feel strange and may scare the patient (Holmstrom et al. 1998). Secondly, one has to be careful and avoid situation when hair around the mouth becomes entangled in a mechanical brush. This author recommends initiating brushing very slowly with a standard toothbrush, and then progressing to a mechanical type after acceptance is achieved.
There are a number of veterinary toothpastes available, 8 which may increase acceptance by the patient ( Figure 5.5). They often contain a calcium chelator 9 in order to decrease the accumulation of dental calculus (Liu et al. 2002; White et al. 2002; Hennet et al. 2007). However, remember that calculus is largely nonpathogenic (Wiggs and Lobprise 1997), so the paste is not a significant player in the reduction of plaque and gingivitis. Consequently, palatability can be increased by using alternative flavorings (Wiggs and Lobprise 1997; Niemiec 2008), such as tuna juice (especially for cats), garlic powder (in small amounts), and beef broth. Dipping the brush in a canned food that the pet enjoys may also be considered on initiation of home brushing.
Читать дальшеИнтервал:
Закладка:
Похожие книги на «The Veterinary Dental Patient: A Multidisciplinary Approach»
Представляем Вашему вниманию похожие книги на «The Veterinary Dental Patient: A Multidisciplinary Approach» списком для выбора. Мы отобрали схожую по названию и смыслу литературу в надежде предоставить читателям больше вариантов отыскать новые, интересные, ещё непрочитанные произведения.








Обсуждение, отзывы о книге «The Veterinary Dental Patient: A Multidisciplinary Approach» и просто собственные мнения читателей. Оставьте ваши комментарии, напишите, что Вы думаете о произведении, его смысле или главных героях. Укажите что конкретно понравилось, а что нет, и почему Вы так считаете.