Ziad Al-Ani - Practical Procedures in Dental Occlusion
Здесь есть возможность читать онлайн «Ziad Al-Ani - Practical Procedures in Dental Occlusion» — ознакомительный отрывок электронной книги совершенно бесплатно, а после прочтения отрывка купить полную версию. В некоторых случаях можно слушать аудио, скачать через торрент в формате fb2 и присутствует краткое содержание. Жанр: unrecognised, на английском языке. Описание произведения, (предисловие) а так же отзывы посетителей доступны на портале библиотеки ЛибКат.
- Название:Practical Procedures in Dental Occlusion
- Автор:
- Жанр:
- Год:неизвестен
- ISBN:нет данных
- Рейтинг книги:3 / 5. Голосов: 1
-
Избранное:Добавить в избранное
- Отзывы:
-
Ваша оценка:
Practical Procedures in Dental Occlusion: краткое содержание, описание и аннотация
Предлагаем к чтению аннотацию, описание, краткое содержание или предисловие (зависит от того, что написал сам автор книги «Practical Procedures in Dental Occlusion»). Если вы не нашли необходимую информацию о книге — напишите в комментариях, мы постараемся отыскать её.
A robust and accessible resource on occlusion for general dental practitioners Practical Procedures in Dental Occlusion
Practical Procedures in Dental Occlusion
Practical Procedures in Dental Occlusion — читать онлайн ознакомительный отрывок
Ниже представлен текст книги, разбитый по страницам. Система сохранения места последней прочитанной страницы, позволяет с удобством читать онлайн бесплатно книгу «Practical Procedures in Dental Occlusion», без необходимости каждый раз заново искать на чём Вы остановились. Поставьте закладку, и сможете в любой момент перейти на страницу, на которой закончили чтение.
Интервал:
Закладка:
Muscles involved in jaw closing (larger muscle mass group underlying where the greater activity is).
Temporalis.
Masseter.
Medial pterygoid
The innervation for these muscles is via the trigeminal nerve (V) but other cranial nerves such as the facial (VII), glossopharyngeal (IX) and hypoglossal (XII) are also involved in the whole process of mastication and swallowing, which comprises more than 30 nerves and muscles (Matsuo and Palmer 2008). Some of these muscles are also involved in respiration and are considered accessory respiratory muscles as discussed by Van Lunteren and Dick (1997).
The pattern of mastication is made up of three successive cycles as described by Lund (1991).
1 The preparatory phase – also called the gathering stage, when the incisors bring the food into the mouth and shift it deeper onto the posterior teeth.
2 The reduction phase – breakdown of food in a rhythm called the chewing cycle; as the food gets smaller, the teeth start to contact, letting us know that the food is ready for swallowing
3 The preswallowing phase – the bolus is prepared for swallowing, the tongue places the food posteriorly and the swallowing reflex is initiated.
The evidence also supports sensory feedback controls for a large part of the masticatory process. Soft foods mean a short masticatory sequence and tough foods provoke a longer sequence, as discussed by Plesh (1986).
Let's look at the sensory feedback system in more detail ( Figure 2.2).
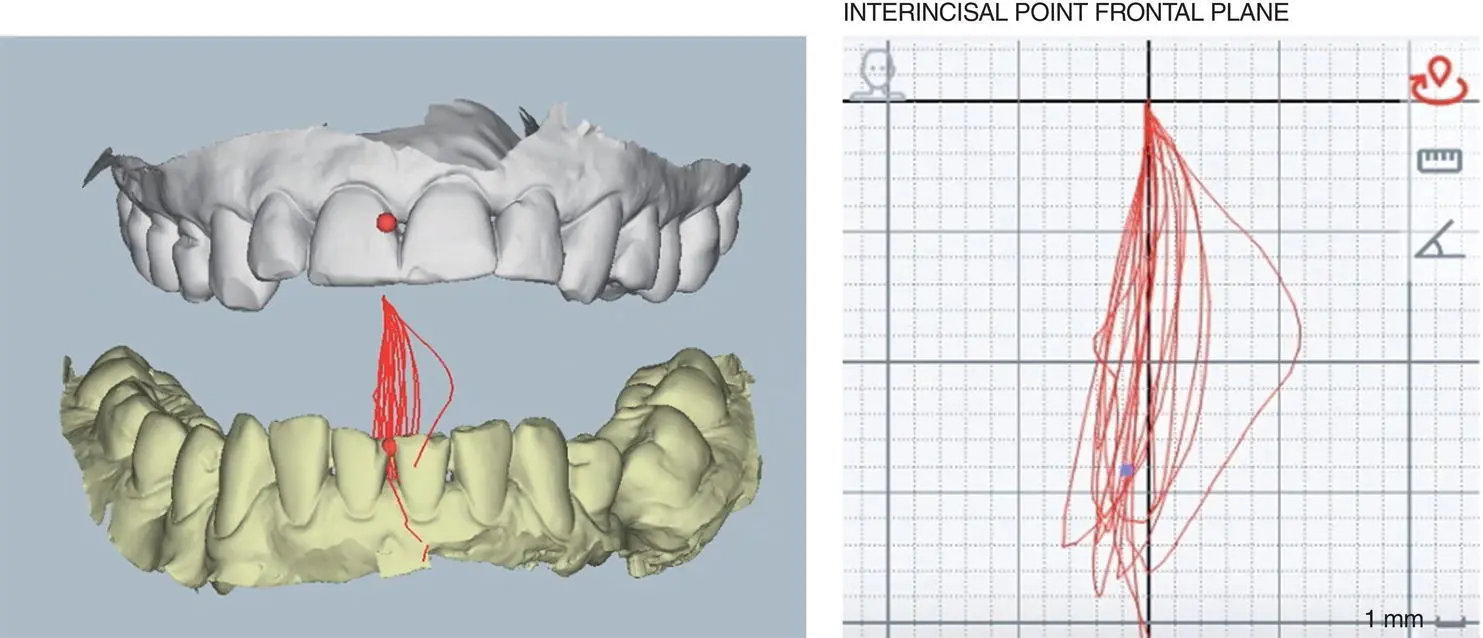
Figure 2.2 Chewing cycle data collected using MODJAW (for further details on MODJAW see Chapter 12).
Sensory and Motor Feedbacks
PDMRs
Situated close to the collagen fibres and in between like a sandwich within the periodontal ligament and described as Ruffini‐like by Byers (1985) and Lambrichts (1992) in humans. The main periodontal Ruffini nerve endings have been classified as type 1 and 2. Type 1 shows lamellar terminal Schwann cells and expanded axon terminals with axonal spines which penetrate surrounding tissue; type 2 is characterised by lesser branched Ruffini endings with fewer axonal spines, less basal lamina and fewer Schwann cells. Both of these receptor types are present in the periodontal ligament (Maeda et al. 1999).These are crucial for force interpretation and control of mastication and therefore it would be assumed that the different teeth (incisors–molars) would have differing sensitivity thresholds and this has been shown to be correct by Johnsen et al. (2007). This is called the interocclusal tactility threshold (ITT) as discussed by Herren (1988) and this study uses foils of varying thickness between healthy teeth. The smallest ITT recorded is between 8 and 60 μm but during chewing the threshold increases by a factor of 5 (range 2.5–8×) and the occlusal perception is reduced due to descending inhibition (sensory gating), meaning there is a filtering out of irrelevant information which allows for enhanced detection of unexpected stimuli. There are also interindividual variations which are ascribed to differing attentional degrees in the higher brain centres and this will be linked to adaptability and neuroplasticity (capability to change and adapt to new demands).
The direction of force also shows that the PDMRs respond more when the forces are axial, i.e. in the direction in which they function best – ‘Directional bias may reflect functional adaptation’ (Sato 1988). When force is applied, the collagen fibrils are compressed which fires the mechanoreceptors. The use of the split and hold tests by Trulsson and Johansson (1996) also determined the amount of force required through a positive feedback loop, meaning the harder the food, the more force is applied through the initial feedback from the mechanoreceptors. A recent systematic review by Piancino et al. (2017) summarises studies that looked at this in greater detail.
What happens, then, when we lose teeth and the PDMRs are lost? Several studies such as Svensson and Trulsson (2011) and Svensson et al. (2013) have shown higher biting and food holding forces, indicating that optimal restoration design is fundamental.
Pulp
The pulp also provides proprioception. Randow and Glanz (1986) showed that non‐vital teeth had mean pain threshold levels that, on cantilever loading, were more than twice as high as those of neighbouring or contralateral vital teeth. This partly explains the vulnerability to fracture of root‐filled teeth.
Muscles
The control of position and movement of the muscle/tendon complex is achieved by a combined Golgi tendon organ (GTO) and muscle spindle (MS) feedback. The jaw closing muscles are richly supplied with MSs which provide information related to length and contraction velocity of muscle fibres and generate muscle activation patterns in a predictable manner. The GTO provides information related to tension of the tendons (Kistemaker et al. 2013). This is a feedback loop system which plays a role in CPGs and given the superior tactile discriminative abilities of dentate subjects in comparison with those with implant‐supported or removable prostheses, PDMRs provide a more sensitive indicator of jaw position and movement.
What happens when we increase the occlusal vertical dimension (OVD)? An increase in OVD results in stretching or increased MS length. Muscles show a high degree of functional adaptability/plasticity; Yabushita et al. (2006) found that there is a significant decrease in MS sensitivity up to 2 weeks post increase of OVD. This has similarities to Clark et al.'s (1999) 68‐year review on occlusal interference studies in that any muscle symptoms were transient. The changes in spindle function may be due to changes in occlusal function producing alterations in CNS masticatory controls combined with the different PDMR input. Therefore, to ensure the information entering the system is correct, assessment of muscles is crucial before embarking on complex reorganised dentistry.
TMJ
The mechanoreceptors in the TMJ joint appear to play a more significant role in providing information in regard to jaw position and movement (Klineberg 1980).
Soft Tissue Receptors
Mucosal and periosteal – these receptors are more important when teeth are lost, i.e. when wearing a complete denture or an implant‐supported prostheses (Jacobs and Van Steenberge 1991).
Cutaneous – the skin contains cutaneous receptors which provide kinaesthetic perceptions, and this has been shown in other parts of the body such as the hand. It is thought that the skin overlying the TMJ may also respond to stretch and therefore provide additional input information regarding condylar movement. There is no direct evidence for this, but we can surmise this during phonetics where the somatosensory input from the facial skin and muscle mechanoreceptors is consistently activated (McClean et al. 1990).
The masticatory system is therefore an all‐encompassing, information‐gathering and communicative neuromuscular system. The term ‘neuromuscular dentistry’ was introduced by Dr Bernard Jankelson in 1967 which helps us understand that the masticatory system is a three‐dimensional system composed of the TMJ, muscles and teeth with a focus on using transcutaneous electrical nerve stimulators (TENS) to stimulate and relax the muscles, thus providing a physiological rest position and the occlusion was then built around this position. There are many other schools of occlusion and they all recognise that we must assess the TMJ and muscles before rebuilding the teeth because an unhealthy joint does not function in the same way as a healthy one.
Читать дальшеИнтервал:
Закладка:
Похожие книги на «Practical Procedures in Dental Occlusion»
Представляем Вашему вниманию похожие книги на «Practical Procedures in Dental Occlusion» списком для выбора. Мы отобрали схожую по названию и смыслу литературу в надежде предоставить читателям больше вариантов отыскать новые, интересные, ещё непрочитанные произведения.






Обсуждение, отзывы о книге «Practical Procedures in Dental Occlusion» и просто собственные мнения читателей. Оставьте ваши комментарии, напишите, что Вы думаете о произведении, его смысле или главных героях. Укажите что конкретно понравилось, а что нет, и почему Вы так считаете.