Douglas A. Terry - Restoring the Intraradicular Space
Здесь есть возможность читать онлайн «Douglas A. Terry - Restoring the Intraradicular Space» — ознакомительный отрывок электронной книги совершенно бесплатно, а после прочтения отрывка купить полную версию. В некоторых случаях можно слушать аудио, скачать через торрент в формате fb2 и присутствует краткое содержание. Жанр: unrecognised, на английском языке. Описание произведения, (предисловие) а так же отзывы посетителей доступны на портале библиотеки ЛибКат.
- Название:Restoring the Intraradicular Space
- Автор:
- Жанр:
- Год:неизвестен
- ISBN:нет данных
- Рейтинг книги:4 / 5. Голосов: 1
-
Избранное:Добавить в избранное
- Отзывы:
-
Ваша оценка:
Restoring the Intraradicular Space: краткое содержание, описание и аннотация
Предлагаем к чтению аннотацию, описание, краткое содержание или предисловие (зависит от того, что написал сам автор книги «Restoring the Intraradicular Space»). Если вы не нашли необходимую информацию о книге — напишите в комментариях, мы постараемся отыскать её.
Restoring the Intraradicular Space — читать онлайн ознакомительный отрывок
Ниже представлен текст книги, разбитый по страницам. Система сохранения места последней прочитанной страницы, позволяет с удобством читать онлайн бесплатно книгу «Restoring the Intraradicular Space», без необходимости каждый раз заново искать на чём Вы остановились. Поставьте закладку, и сможете в любой момент перейти на страницу, на которой закончили чтение.
Интервал:
Закладка:
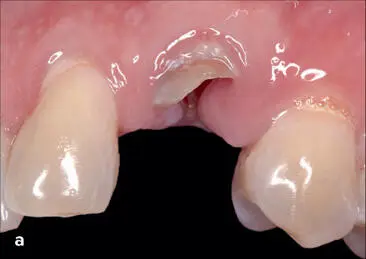







Fig 1-22 (a and b) The patient presented with a subgingival fracture of the maxillary left canine with caries. (c) After anesthesia, bone sounding confirmed that gingival resection would provide an adequate ferrule without infringing on the biologic width. A treatment plan was discussed with the patient that included crown lengthening of the canine to establish a ferrule effect of 1 to 2 mm, endodontic therapy, and placement of a fiber-reinforced post and core as well as an all-ceramic restoration. (d) Before restorative treatment was initiated, a gingivectomy was performed to gain sound coronal tooth structure. (e) After endodontic therapy was performed, a fiber-reinforced post and core was completed. (f) The provisional restoration (G-aenial Universal Flo) was fabricated from a clear matrix of the diagnostic wax-up using a polyvinyl siloxane impression material (Exaclear, GC America). The provisional restoration was fabricated intraorally using the inverse injection-layering technique, using A1- and B1-shaded flowable resin composite (G-aenial Universal Flo). The provisional restoration guided the tissue shaping and required 3 months to develop the emergence profile. (g) The completed zirconia ceramic crown on the maxillary left canine. (h) Note the healthy biologic framework and the integration of color with the adjacent dentition.




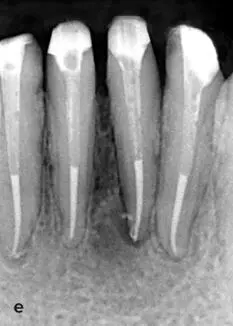
Fig 1-23 Mandibular crown lengthening in a case of severe tooth attrition and secondary dental caries (a) , with healthy periodontal support. (b) The mandibular canines and incisors were treated endodontically. The crown lengthening procedure was performed with a buccal full-thickness flap and interproximal papillae retention. The osseous crown lengthening exposed healthy root structure in adequate amounts to establish the anticipated and predetermined preparation margins. (c) The flap was apically positioned and sutured with nonresorbable sutures. (d and e) Healing and maturation of the gingivoperiodontal complex at 3 months. Fiber-reinforced composite posts were placed using the adhesive design concept, and the patient is ready for restorative treatment. (Dentistry courtesy of Islam S. Zakzouk, BDS.)
Orthodontic extrusion
Orthodontic extrusion614 ,615 or forced eruption procedures can also be used to provide access for treatment of subgingival caries, fractures, or defective restorations and for establishing an optimal restorative dimension583 ,598 ,615 –617 ( Figs 1-24to 1-26). This method provides a controlled extrusion of the fractured tooth by utilizing a gentle, continuous force to effect changes in hard and soft tissues. It is predominantly used in the anterior region where esthetic concerns are paramount. An extrusion technique can be achieved with fixed or removable appliances with various kinds attachments such as stainless steel hooks, brackets, magnets,608 ,618 composite buttons, and surgical controlled extrusion with a mechanical screw device (Benex System).608 ,619 –621 Factors to consider prior to performing this procedure include oral hygiene, periodontal condition, caries index, tooth position, root proximity, morphology, restorability, occlusion, and esthetics.606 Clinical reports indicate there is approximately 1 mm of coronal movement every 1.5 weeks, and stabilization is required.585 With this procedure, the biomechanical principle of relapse can occur603 ,622; therefore, it is recommended that there should be 1 month of stabilization for every millimeter of extrusion.605 ,606 This method is considered an alternative to the surgical approach585; however, crown lengthening may be required after forced extrusion of the tooth because attached gingiva and alveolar bone can move coronally during the event.585 ,591 ,597 ,598 ,606 ,623 –627 However, the more rapid the movement, the less likely one will extrude the supporting structures. Generally, this process requires a period of 6 to 8 weeks for treatment and to stabilize with a fixed appliance. To prevent coronal movement of gingival tissue and alveolar bone during the eruption and post procedure, supracrestal fiberotomies have been recommended587 ,591 ,601 ,614 ,618 ,628 ,629 once a week during the movement and post procedure to stabilize and prevent relapse.629 This procedure requires severing the supracrestal periodontal fibers with a periotome or narrow-bladed scalpel, thus reducing the tensile strength in the hard and soft tissues during tooth extrusion.587 ,591 ,618
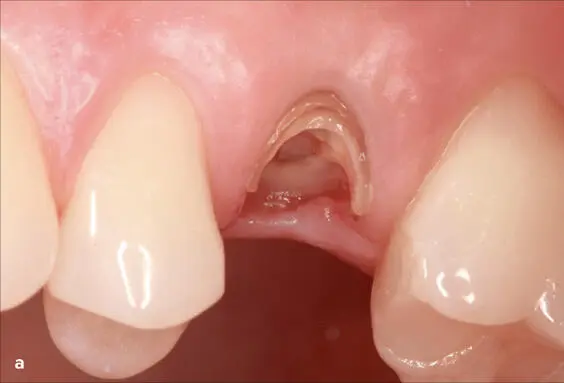

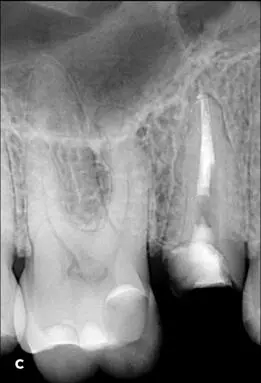





Fig 1-24 (a and b) Orthodontic extrusion can be used to provide access for treatment of this subgingival caries and for establishing an optimal restorative dimension. (c) After careful caries removal and endodontic retreatment of the maxillary right second premolar, two fiber posts were adhesively cemented. (d) An orthodontic bracket was positioned on the buccal aspect of the premolar. (e and f) To prevent coronal movement of gingival tissue and alveolar bone during the eruption and post procedure, supracrestal fiberotomies were performed once per week to stabilize and prevent relapse. (g) Completed post and core preparation after stabilization for 2 months. (h) Final radiograph depicting the restorative margin coronal to the supracrestal apparatus, which is crucial for long-term success of the restoration. (Dentistry courtesy of Maciej Zarow, DDS, PhD.)
Читать дальшеИнтервал:
Закладка:
Похожие книги на «Restoring the Intraradicular Space»
Представляем Вашему вниманию похожие книги на «Restoring the Intraradicular Space» списком для выбора. Мы отобрали схожую по названию и смыслу литературу в надежде предоставить читателям больше вариантов отыскать новые, интересные, ещё непрочитанные произведения.




Обсуждение, отзывы о книге «Restoring the Intraradicular Space» и просто собственные мнения читателей. Оставьте ваши комментарии, напишите, что Вы думаете о произведении, его смысле или главных героях. Укажите что конкретно понравилось, а что нет, и почему Вы так считаете.