Clinical Dilemmas in Diabetes
Здесь есть возможность читать онлайн «Clinical Dilemmas in Diabetes» — ознакомительный отрывок электронной книги совершенно бесплатно, а после прочтения отрывка купить полную версию. В некоторых случаях можно слушать аудио, скачать через торрент в формате fb2 и присутствует краткое содержание. Жанр: unrecognised, на английском языке. Описание произведения, (предисловие) а так же отзывы посетителей доступны на портале библиотеки ЛибКат.
- Название:Clinical Dilemmas in Diabetes
- Автор:
- Жанр:
- Год:неизвестен
- ISBN:нет данных
- Рейтинг книги:4 / 5. Голосов: 1
-
Избранное:Добавить в избранное
- Отзывы:
-
Ваша оценка:
Clinical Dilemmas in Diabetes: краткое содержание, описание и аннотация
Предлагаем к чтению аннотацию, описание, краткое содержание или предисловие (зависит от того, что написал сам автор книги «Clinical Dilemmas in Diabetes»). Если вы не нашли необходимую информацию о книге — напишите в комментариях, мы постараемся отыскать её.
contains extensively reviewed and revised information throughout. New and updated chapters examine prediction, diagnosis, and management of early Type 1 diabetes, ophthalmic complications, screening asymptomatic patients for cardiovascular disease, new agents for treatment of dyslipidemia, closed loop systems in Type 1 diabetes, upper gastrointestinal manifestations, managing hyperglycemia in critically ill patients, and more. Edited by Dr. Vella at the Mayo Clinic, this highly practical resource:
Encourages evidence-based clinical decision-making, rather than algorithm-based approaches Provides clear guidance on common problematic areas, especially in cases where conflicts in treatment for the disease and the complications occur Emphasizes the importance of translating the results of clinical trials to individual care and management of diabetes Contains effective learning and revision tools, including Learning Points, chapter introductions and summaries, tables and figures, color diagrams and charts, and full references Part of the popular
series,
is a must-have guide for anyone involved in the treatment of patients with diabetes, particularly endocrinologists, diabetes specialists and consultants, cardiologists, residents, fellows, specialist nurses, and general practitioners with an interest in diabetes.
Clinical Dilemmas in Diabetes — читать онлайн ознакомительный отрывок
Ниже представлен текст книги, разбитый по страницам. Система сохранения места последней прочитанной страницы, позволяет с удобством читать онлайн бесплатно книгу «Clinical Dilemmas in Diabetes», без необходимости каждый раз заново искать на чём Вы остановились. Поставьте закладку, и сможете в любой момент перейти на страницу, на которой закончили чтение.
Интервал:
Закладка:
Numerous clinical trials have attempted to change the course of disease or prevent its onset. Of these, early immune intervention holds the most promise.
Introduction
Type 1 diabetes (T1D) is one of the most widespread chronic disease occurring in children and young adults. In 2001, people with diabetes (all types included) were 177 million worldwide, in 2010 285 million, in 2019 approximately 463 million and it is predicted that some 700 million people worldwide will live with diabetes in 2045 [1].
As the prevalence of diabetes continues to rise worldwide, disease‐related morbidity and mortality are emerging as major healthcare problems. Epidemiologic data show that diabetes‐related long‐term complications begin early in the natural history of the disease . These findings indicate that early identification and management of individuals at increased risk of T1D has the potential to reduce both the clinical onset of the disease and its related complications.
The global incidence of T1D in children and adolescents is rising with an estimated overall annual increase of approximately 3%. These recent epidemiologic trends in T1D have been shown in countries having both high and low prevalence figures, with an indication of a steeper increase in some of the low‐prevalence countries. T1D accounts for about 10% of all cases of diabetes, occurs most commonly in people of European descent and affects 2 million people in Europe and North America [1]. The lowest incidence has been found in Asia and Oceania, the highest in Europe.
As far as its pathogenesis is concerned, T1D results from the autoimmune destruction of pancreatic insulin‐secreting β‐cells. Genetic, metabolic, and environmental factors act together to precipitate the onset of the disease. The excess mortality associated with diabetes‐related complications and the increasing prevalence of the disease among the youth, emphasize the importance of novel therapeutic strategies to prevent or slow down the autoimmune process.
Pathogenesis of T1D: An Update in View of Defining Preventive Tools
There are three main categories of factors involved in the pathogenesis of T1D. These are genetic, immunological, and environmental factors ( Figure 2.1).
Like other organ‐specific autoimmune diseases, T1D shows specific human leukocyte antigen (HLA) associations. The HLA complex on chromosome 6 comprises the first gene shown to be associated with the disease and it is considered to contribute to almost half of the familial basis of T1D. Two combinations of HLA haplotypes are of particular importance. They are DR4‐DQ8 and DR3‐DQ2, which are present in 90% of children with T1D [5]. A third haplotype, DR15‐DQ6, is found in less than 1% of children with T1D, compared to more than 20% of the general population, and it is considered to be protective. The genotype combining the two susceptibility haplotypes (DR4‐DQ8/DR3‐DQ2) contributes to the greatest risk of the disease and it appears frequently in children with an earlier onset. First‐degree relatives of these children are themselves at greater risk of T1D compared to those of children in whom the disease develops later.
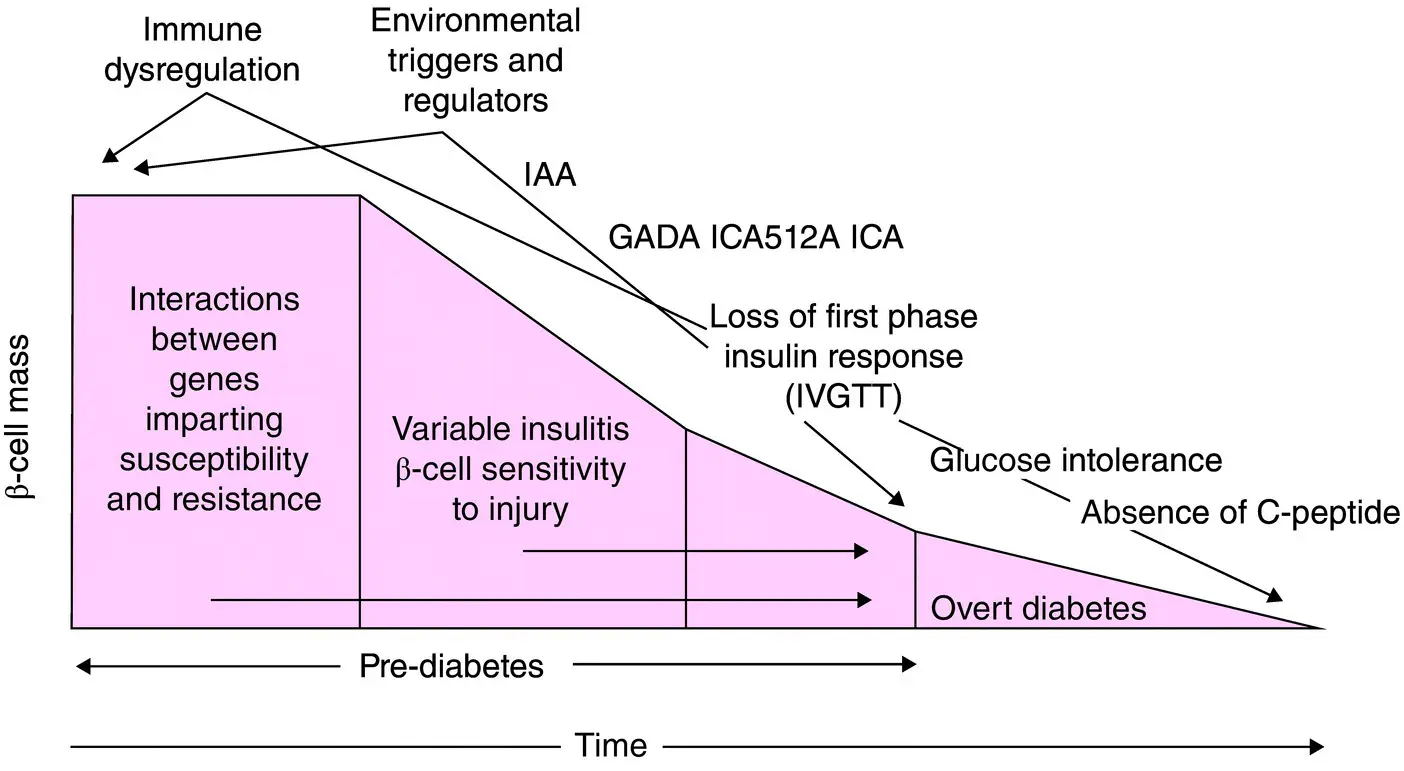
FIG 2.1 Pathogenesis and natural history of Type 1 diabetes. Atkinson MA and Eisenbarth GS Type 1 diabetes: new perspectives on disease pathogenesis and treatment. Lancet 2001;358(9277):221–229.
Candidate gene studies also identified the insulin gene on chromosome 11 as another important genetic susceptibility factor, contributing 10% of the genetic susceptibility to T1D [6]. Similarly, an allele of the gene acting as a negative regulator of T‐cell activation, cytotoxic T lymphocyte antigen 4 (CTLA‐4), found on chromosome 2q33, is considered to be another susceptibility gene for T1D [7]. A variant of PTPN22 , the gene encoding Lymphoid Phosphatase (LYP), which is a suppressor of T‐cell activation, has been deemed as another susceptibility gene [8]. Similarly, variation in IL2RA which encodes the α‐chain of the IL‐2 receptor is also associated with T1D [9]. The observation that these susceptibility genes for T1D all play important roles in antigen presentation to T‐cells, emphasizes the potential importance of current therapeutic strategies targeting this interaction [10].
Genetic studies have highlighted the importance of large, well‐characterized populations in the identification of susceptibility genes for T1D. Recruitment of increasingly large populations of patients with T1D and their families is required to provide statistically powerful cohorts in which to identify other disease‐associated genes. Some genes have a relatively minor individual impact on susceptibility to disease but could nevertheless provide more clues to future preventive therapies.
The presence of autoantibodies to β‐cells is the hallmark of T1D ( Figure 2.1). Abnormal activation of the T‐cell‐mediated immune system in susceptible individuals leads to an inflammatory response within the islets as well as to a humoral response with production of antibodies to β‐cell antigens. Islet‐cell antibodies (ICA) were the first ones described, followed by more specific autoantibodies to insulin (IAA), glutamic acid decarboxylase (GAD), the protein tyrosine phosphatase (IA‐2), and most recently Zinc Transporter 8 (ZnT8A), all of which can be easily detected by sensitive radioimmunoassay to identify subjects at risk of developing T1D [11]. These autoantibodies are common in both childhood and adult onset T1D, with many subjects being positive for multiple autoantibodies. The type of immune response is age‐dependent, but seroconversion to multiple autoantibody positivity usually occurs tightly clustered in time and is associated with genetic risk.
The presence of one or more type of antibodies can precede the clinical onset of T1D by years or even decades. These autoantibodies are usually persistent, although a small group of individuals may revert to being seronegative without progressing to clinical diabetes. The presence and persistence of positivity to multiple antibodies increases the likelihood of progression to clinical disease.
On that note, recent evidence shows that antibodies specific to oxidative post‐translationally modified insulin (oxPTM‐INS) are present in the majority of newly diagnosed individuals with T1D being significantly more abundant than autoantibodies to native insulin (NT‐INS) [12]. Furthermore, subsequent analysis found that oxPTM‐INS auto‐reactivity is present before diabetes diagnosis in over 90% of individuals, suggesting a potential role for oxPTM‐INS‐Ab as a predictive biomarker of T1D [13].
The progressive reduction of insulin‐secretory reserve leads primarily to the loss of the first phase insulin secretion in response to an intravenous glucose tolerance test, and therefore to a state of absolute insulin deficiency.
Regarding the role of environmental factors, it should be underlined that the increase in incidence of T1D is too rapid to be caused by alterations in the genetic background and is likely to be the result of environmental changes.
What Are the Environmental Factors Triggering Type 1 Diabetes?
Certain viral infections may play a role in the pathogenesis of human T1D. Congenital rubella is the classical example of virus‐induced diabetes in human beings, but effective immunization programs have eliminated congenital rubella in most Western countries. Currently, the main candidate for a viral trigger of human diabetes is members of the group of Enterovirus [14]. They are small non‐enveloped RNA viruses, which belong to the Picornavirus family. They consist of more than 60 different serotypes, with the Polioviruses being their best‐known representatives. Enterovirus infections are frequent among children and adolescents causing aseptic meningitis, myocarditis, rash, hand‐food‐and‐mouth disease, paralysis, respiratory infections, and severe systemic infections in newborn infants. Most infections, however, are subclinical or manifest with mild respiratory symptoms. The primary replication of the virus occurs in the lymphoid tissues of the pharynx and small intestine, and during the following viremic phase the virus can spread to various organs including the β‐cells.
Читать дальшеИнтервал:
Закладка:
Похожие книги на «Clinical Dilemmas in Diabetes»
Представляем Вашему вниманию похожие книги на «Clinical Dilemmas in Diabetes» списком для выбора. Мы отобрали схожую по названию и смыслу литературу в надежде предоставить читателям больше вариантов отыскать новые, интересные, ещё непрочитанные произведения.






Обсуждение, отзывы о книге «Clinical Dilemmas in Diabetes» и просто собственные мнения читателей. Оставьте ваши комментарии, напишите, что Вы думаете о произведении, его смысле или главных героях. Укажите что конкретно понравилось, а что нет, и почему Вы так считаете.