Bone and Soft Tissue Augmentation in Implantology
Здесь есть возможность читать онлайн «Bone and Soft Tissue Augmentation in Implantology» — ознакомительный отрывок электронной книги совершенно бесплатно, а после прочтения отрывка купить полную версию. В некоторых случаях можно слушать аудио, скачать через торрент в формате fb2 и присутствует краткое содержание. Жанр: unrecognised, на английском языке. Описание произведения, (предисловие) а так же отзывы посетителей доступны на портале библиотеки ЛибКат.
- Название:Bone and Soft Tissue Augmentation in Implantology
- Автор:
- Жанр:
- Год:неизвестен
- ISBN:нет данных
- Рейтинг книги:4 / 5. Голосов: 1
-
Избранное:Добавить в избранное
- Отзывы:
-
Ваша оценка:
Bone and Soft Tissue Augmentation in Implantology: краткое содержание, описание и аннотация
Предлагаем к чтению аннотацию, описание, краткое содержание или предисловие (зависит от того, что написал сам автор книги «Bone and Soft Tissue Augmentation in Implantology»). Если вы не нашли необходимую информацию о книге — напишите в комментариях, мы постараемся отыскать её.
R. Gruber, Th. Hanser, Ph. Keeve, Ch. Khoury, J. Neugebauer, J. E. Zöller
Bone and Soft Tissue Augmentation in Implantology addresses useful methods of bone grafting procedures in implant treatment based on current biologic principles and constitutes a unique reference in this field. The book describes, in over 760 pages and 2837 mostly color illustrations, the different possibilities available to augment the bone volume in width and height. The information presented includes not only the underlying scientific concepts of the different augmentation techniques with autogenous bone, but also the associated soft tissue management, from safe approaches to different possibilities for soft tissue augmentation and papilla reconstruction techniques.
The book provides surgeons with a basic understanding of the biologic response to bone grafting procedures. Experienced implantologists will benefit from the in-depth background information, details of high-level surgical techniques, and scientific results, which will enable them to optimize their surgical procedures. Each chapter offers a wealth of information on the specific topic covered, with much attention given to the scientific concepts behind each one. Extensive case reports with step-by-step documentation allow readers to gain an impression of what is possible today in the 3D reconstruction procedures of the alveolar crest. Important criteria for success are presented as well as possible complications and their treatment.
Bone and Soft Tissue Augmentation in Implantology is a must-read for every implantologist, oral and maxillofacial surgeon, and any dentist interested in surgery.
Bone and Soft Tissue Augmentation in Implantology — читать онлайн ознакомительный отрывок
Ниже представлен текст книги, разбитый по страницам. Система сохранения места последней прочитанной страницы, позволяет с удобством читать онлайн бесплатно книгу «Bone and Soft Tissue Augmentation in Implantology», без необходимости каждый раз заново искать на чём Вы остановились. Поставьте закладку, и сможете в любой момент перейти на страницу, на которой закончили чтение.
Интервал:
Закладка:
The planning of the position, number, and dimension of the implants represents the essential step for a successful restoration from an esthetic and functional point of view. The prosthetic aspects have to be considered and the available bone evaluated. Today, implants can be inserted from a prosthetic point of view as far as possible using various grafting techniques. 81Nevertheless, it is necessary to take precise account of the anatomical landmarks at the time of implant placement, 44otherwise insufficient bony coverage of the implant surface can lead to complications such as peri-implantitis shortly after the final prosthetic delivery. 29Further restrictions in terms of the functionality of the prosthetic restoration result from implant positions that require a non-physiologic tooth shape with a limited esthetic result ( Fig 2-1ato d) or do not allow for sufficient hygiene maintenance ( Fig 2-2ato g). 94

Fig 2-1aLong crown after deep implant placement without considering a two-stage grafting procedure.

Fig 2-1bNon-physiologic crown shape with limited oral hygiene options.

Fig 2-1cFailed implant restoration in the maxillary anterior area.
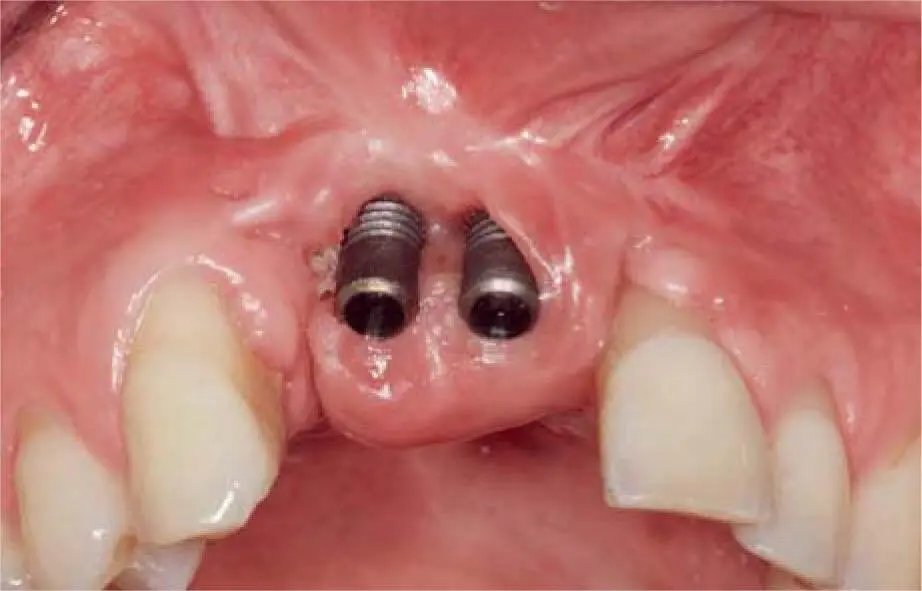
Fig 2-1dClinical situation after removal of the crowns.

Fig 2-2aClinical aspect of an unesthetic and unhygienic restoration.
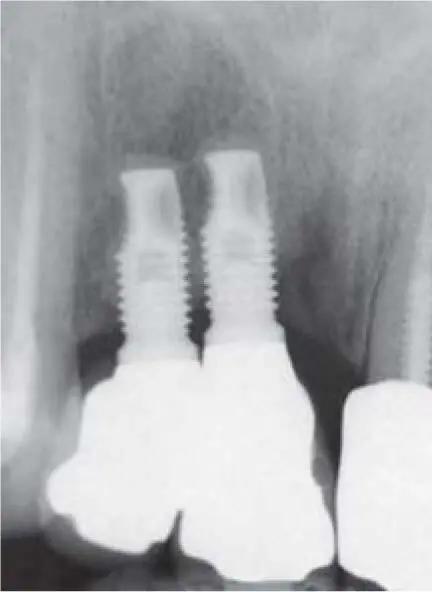
Fig 2-2bMinimal implant distance as the cause of an unacceptable result.

Fig 2-2cDirect contact of two implants prevents the formation of interimplant soft tissue.
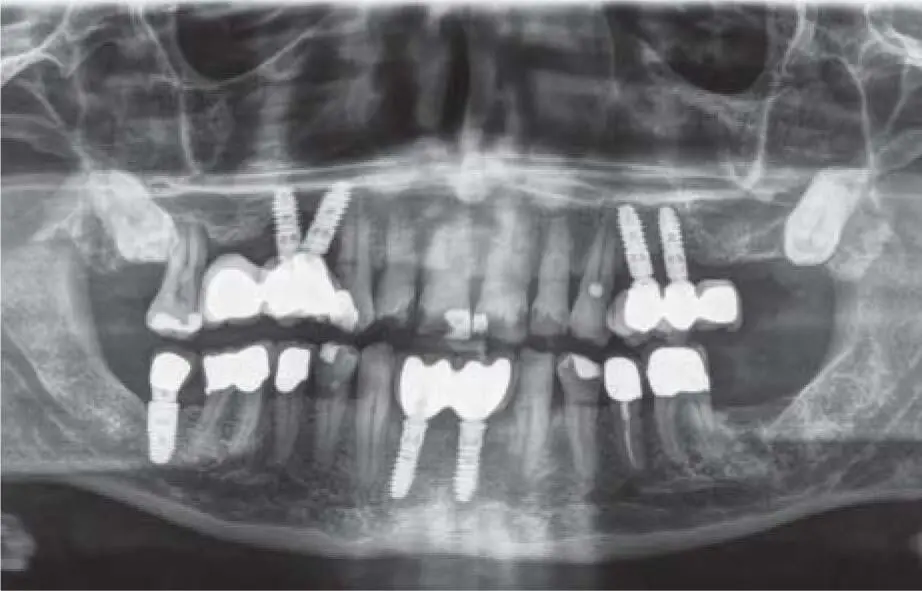
Fig 2-2dPanoramic radiograph documenting bad implant planning especially in the right maxilla, leading to peri-implant bone loss.

Fig 2-2eClinical aspect of Figure 2-2d, documenting unesthetic and unhygienic restorations due to bad implant positions.

Fig 2-2fClinical situation in the right maxilla offering inadequate cleaning possibility.
2.2 Patient consultation
Depending on the patient’s expectations and willingness to cooperate, it is necessary to precisely define the aim of the treatment. Clarify right from the start in detail the various available grafting techniques and their suitability for the specific patient. Also, alternative methods should be considered such as diameter-reduced or ultrashort and tilted implant placement to avoid grafting procedures. 69,77To achieve the best possible patient cooperation and satisfaction, it is not sufficient to only explain the intra- and postoperative surgical risks. Patients need information about the overall treatment duration, costs involved, and possible alternative procedures. 77During the course of clarifying the implant prosthetic treatment requirements and procedures, it may happen that the patient’s original expectations change once the realization sinks in that the time involved, the material costs, the surgical procedure itself or the increased risks of surgery, especially in the presence of systemic disease, are too much for the patient.
Especially in patients with alveolar crest defects, it is important to describe the entire treatment at the beginning. To achieve high patient satisfaction, it is vital to match the patient’s expectations and the necessary treatment steps as closely as possible. 8

Fig 2-2gClinical situation in the left maxilla showing exposed implant neck due to lack of bone and soft tissue.
For the definition of the selected therapy, special attention should be paid to the motivation of the patient in an extensive implant prosthetic treatment in order to achieve good cooperation in the long-lasting and intensive course of therapy. Important information about the patient’s motivation is provided by the cause of the tooth loss and the patient’s attitude toward it ( Fig 2-3aand b). The possibilities of the prosthetic design also depend on the awareness of the patient regarding hygiene. Depending on the patient’s oral hygiene status, the choice between fixed, conditionally removable, and removable prostheses should be differentiated.
2.3 Anamnesis
In addition to the general conditions, the medication, the presence of allergies, the consumption of psychoactive drugs, and the patient’s attitude to antibiotic medication should be surveyed as part of the medical history. In particular, there is a tendency of differentiated patients to reject a postoperative antibiotic medication, which can lead to an increased complication rate, especially when using heterologous grafting materials.

Fig 2-3aPeriodontally compromised dentition with non-restorable teeth in the maxilla and a pronounced gagging reflex.
2.3.1 Nicotine consumption
Patients often show early tooth loss due to nicotine use. This situation should be rehabilitated by correspondingly extensive therapies with a fixed prosthesis. 52Tobacco smoke passing through the oral cavity contains a mixture of hazardous substances that has cytotoxic and carcinogenic effects. This leads to a degeneration of the soft tissue, with a reduced perfusion and vascular supply, which, in a similar way to diabetes mellitus, can lead to surgical or long-term complications in implant therapy. 46
If patients show complete or partial tooth loss with pronounced or severe alveolar ridge atrophy at the end of the fourth decade of life, an evaluation of the interleukin-1 polymorphism can be made. This is synergistically known in smokers for chronic periodontal disease. At the same time, these patients also have an increased risk of peri-implantitis. 11,32In order to clarify the long-term prognosis, simple swab tests are now commercially available that allow the pain-free diagnosis of an IL-1 mutation by polymerase chain reaction (PCR)-based methods.
Читать дальшеИнтервал:
Закладка:
Похожие книги на «Bone and Soft Tissue Augmentation in Implantology»
Представляем Вашему вниманию похожие книги на «Bone and Soft Tissue Augmentation in Implantology» списком для выбора. Мы отобрали схожую по названию и смыслу литературу в надежде предоставить читателям больше вариантов отыскать новые, интересные, ещё непрочитанные произведения.







Обсуждение, отзывы о книге «Bone and Soft Tissue Augmentation in Implantology» и просто собственные мнения читателей. Оставьте ваши комментарии, напишите, что Вы думаете о произведении, его смысле или главных героях. Укажите что конкретно понравилось, а что нет, и почему Вы так считаете.