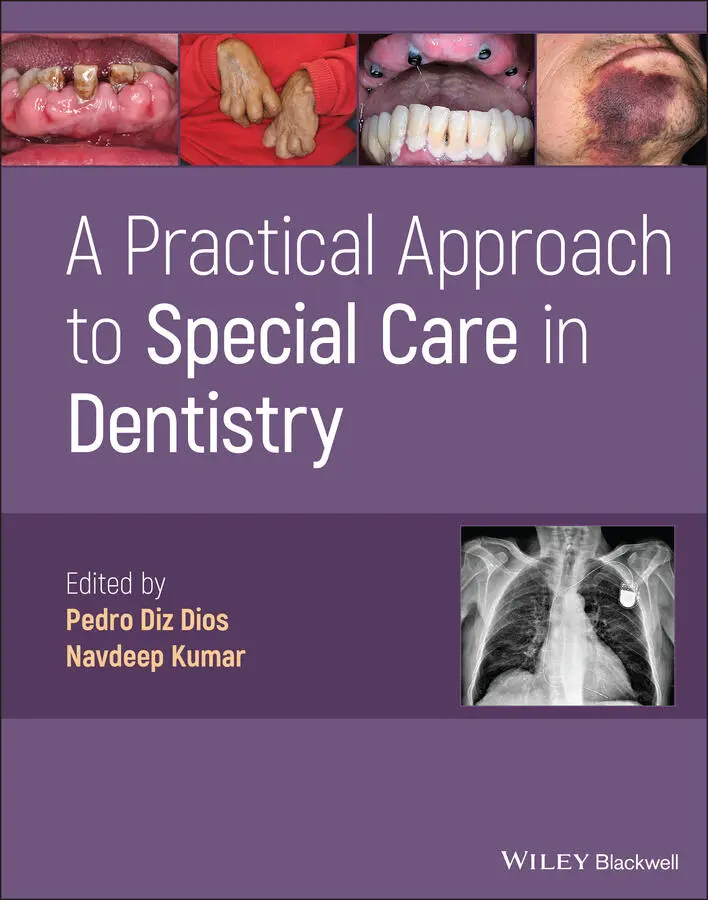
A Practical Approach to Special Care in Dentistry
Здесь есть возможность читать онлайн «A Practical Approach to Special Care in Dentistry» — ознакомительный отрывок электронной книги совершенно бесплатно, а после прочтения отрывка купить полную версию. В некоторых случаях можно слушать аудио, скачать через торрент в формате fb2 и присутствует краткое содержание. Жанр: unrecognised, на английском языке. Описание произведения, (предисловие) а так же отзывы посетителей доступны на портале библиотеки ЛибКат.
- Название:A Practical Approach to Special Care in Dentistry
- Автор:
- Жанр:
- Год:неизвестен
- ISBN:нет данных
- Рейтинг книги:3 / 5. Голосов: 1
-
Избранное:Добавить в избранное
- Отзывы:
-
Ваша оценка:
A Practical Approach to Special Care in Dentistry: краткое содержание, описание и аннотация
Предлагаем к чтению аннотацию, описание, краткое содержание или предисловие (зависит от того, что написал сам автор книги «A Practical Approach to Special Care in Dentistry»). Если вы не нашли необходимую информацию о книге — напишите в комментариях, мы постараемся отыскать её.
Learn to treat dental patients with disabilities or who are medically compromised A Practical Approach to Special Care in Dentistry
A Practical Approach to Special Care in Dentistry
A Practical Approach to Special Care in Dentistry — читать онлайн ознакомительный отрывок
Ниже представлен текст книги, разбитый по страницам. Система сохранения места последней прочитанной страницы, позволяет с удобством читать онлайн бесплатно книгу «A Practical Approach to Special Care in Dentistry», без необходимости каждый раз заново искать на чём Вы остановились. Поставьте закладку, и сможете в любой момент перейти на страницу, на которой закончили чтение.
Интервал:
Закладка:
5 The patient requests oral prosthetic rehabilitation after her teeth are extracted/stabilised. What options would you discuss?If oral hygiene improves:Removable prostheses can be difficult to insert and, with oral dyskinesias, are more unstable, potentially causing injuries to the mucosa/obstruction of the airway if dislodgedFixed implant‐supported or tooth‐supported prostheses are preferable; these can be limited to the anterior/aesthetic zones to allow for improved appearance and easier access for cleaningThe cost of these options needs to be consideredIf oral hygiene remains poor and the dental caries risk remains high:It may be preferable to accept the gaps rather than compromise further teethAlternatively, a removable dental prosthesis may be attempted as this is reversible and can be removed to allow access for cleaningFurthermore, teeth can be added to the partial denture, if further dental extractions become necessaryThis may be better than implant‐supported measures if there are financial limitations
6 Drooling (sialorrhoea) is a common consequence of cerebral palsy among patients with difficulties swallowing saliva. What medication is this patient taking that could be of benefit?Trihexyphenidyl hydrochloride is an anticholinergic drug and hence reduces saliva productionThis medication may also be effective for reducing dystonia or improving upper arm function in patients with cerebral palsy
7 What are the most widely used therapeutic modalities for sialorrhoea?Physiotherapy for swallowing and postural re‐educationDrugs: anticholinergic agents (scopolamine, atropine, glycopyrrolate) or botulinum toxinSurgery: Wharton's duct relocation, excision of a submandibular gland or selective neurectomy
General Dental Considerations
Oral Findings
Delayed eruption of primary dentition
Enamel hypoplasia
Bruxism and abnormal dental attrition
Gingivitis and periodontal disease
Anterior tooth trauma due to falls
Spontaneous dislocation or subluxation of the temporomandibular joint
Malocclusion (anterior open bite and Angle class II‐1) ( Figure 1.1.3a)
Sialorrhoea/drooling, promoted by the head position and difficulties swallowing saliva ( Figure 1.1.3b)
Dental Management ( Figure 1.1.4)
The dental treatment plan is determined more by the disease severity (e.g. severity of the spasticity) and its comorbidities (e.g. respiratory impairment) than by the type of cerebral palsy ( Table 1.1.1)
Dental manipulation and stress can intensify the uncontrolled movements
Section II: Background Information and Guidelines
Definition
Cerebral palsy is a group of permanent disorders of the development of movement and posture, resulting from non‐progressive disturbances (structural abnormalities) that occurred in the developing foetal or infant brain. It is the most common form of chronic motor disability in childhood, with an estimated prevalence of 2.0–3.5 cases per 1000 live births in developed countries.

Figure 1.1.3 (a) Severe malocclusion with anterior open bite. (b) Sialorrhoea/drooling.
Aetiopathogenesis
The condition is attributed to structural brain abnormalities and hypoxia due to cerebrovascular insufficiency
This may occur during the prenatal, perinatal or postnatal periodsPrenatal: infections, exposure to toxins and multiple pregnanciesPerinatal: traumatic births and prematurity (especially for infants weighing less than 2500 g)Postnatal: infections, intracranial haemorrhages and kernicterus
Clinical Presentation
Cerebral palsy is subdivided into spastic, dyskinetic (including dystonic) and ataxic forms, depending on the area of the brain that is mainly involved ( Table 1.1.2; Figure 1.1.5) Figure 1.1.4 Patients who present in wheelchairs may have treatment provided without transfer.
In over 50% of patients, it is accompanied by disturbances of sensation (visual and auditory defects), perception, cognition, communication and behaviour
Epilepsy and musculoskeletal problems may also be present
Diagnosis
There are no specific tests to confirm or eliminate the diagnosis of cerebral palsy
The suspected diagnosis is based on clinical findings and the failure to reach appropriate developmental milestones for the patient's age
There is general consensus of an upper age limit of 2 years for the onset of the non‐progressive brain disturbance and five years for a clinical or developmental diagnosis
Diagnostic brain imaging tests, including computed tomography and magnetic resonance imaging, can be of use
An electroencephalogram, genetic analysis and metabolic tests may also be undertaken
Management
Physical therapy and occasionally orthopaedic surgery Table 1.1.1 Considerations for dental management.Risk assessmentInvoluntary movements and contractions – these can increase further with stress and local stimuliAbnormal gag/bite reflexAbnormal swallowing and cough reflexAspiration riskEpilepsyCriteria for referralReferral to a specialised clinic or hospital centre is determined by:Factors related to the severity of the patient's general condition (e.g. respiratory distress, uncontrolled seizures)Factors that significantly limit access for dental procedures (e.g. pathological reflexes and uncontrolled movements)Access/positionPatients who present in wheelchairs may have treatment provided without transfer, particularly if there is a wheelchair platform available ( Figure 1.1.4)If they are transferred to the dental chair, the patients will need to be stabilised with pillowsConsider safe immobilisation of the head using vacuum cushions/supports with consentCommunicationFrequent difficulties in verbal communicationNon‐verbal language might sometimes need to be interpretedThe level of comprehension can be normalConcentration may be poorConsent/capacityCapacity may be intactDo not make assumptions due to the physical signs/symptoms or impaired verbal communicationClinical holding may be required (e.g. to reduce involuntary arm movements) – this must be appropriately risk assessed, undertaken by trained staff, consented and documentedRegular medication may be sedative and hence impair capacityAnaesthesia/sedationLocal anaesthesiaNot contraindicated, although involuntary movements may make delivery challengingSedationConscious sedation can help control anxiety, nausea and lingual dystoniaMedical consultation is recommended if the patient takes neuroleptics, is already taking benzodiazepines or has respiratory difficultiesGeneral anaesthesiaMay be indicated if the movements are uncontrollable or there is a lack of co‐operation (the risk/benefit should be assessed)Dental treatmentBeforeThe need for conscious sedation should be anticipated and consent for any intervention undertaken prior to thisOrthodontic treatment planning should consider the impact of increased muscle toneDuringConsider the use of atraumatic mouth openers, protective thimbles and stainless steel/plastic mirrors (involuntary contractions)Fixed prostheses are generally preferable over removable prostheses (due to difficulties inserting the prosthesis, involuntary movements and the risk of fracture in patients with epilepsy)AfterClose follow‐up after completion of orthodontic therapy as relapse is more frequentDrug prescriptionConsider the associated systemic complications and concurrent medicationsCaution with the use of benzodiazepines if the patient is already taking sedation medicationEducation/preventionInvolve the relatives and caregivers where possibleAn electric or adapted manual toothbrush should be consideredRegular oral prophylaxis/calculus removalFluoride treatmentDietary counselling Table 1.1.2 Classification and characteristics of cerebral palsy.Type (lesion location)FrequencyClinical presentationSubtype/area involvedSpastic (upper motor neuron) 70–80%Muscle hypertonia Contracture HyperreflexiaMonoplegic: one extremityParaplegic: legsHemiplegic: one arm and one ipsilateral legDouble hemiplegic: all extremities but more in the armsDiplegic: all extremities but more in the legsTetraplegic: all extremitiesAthetoid (basal ganglia) 15%Vermiform movements Muscle hypertoniaChorea (restless, fidgety, dancing movement): face, chest and extremitiesAthetosis (slow, writhing movement): hands and feetChoreoathetosis: generalisedAtaxic (cerebellum) 10%Abnormal equilibrium and gait
Читать дальшеИнтервал:
Закладка:
Похожие книги на «A Practical Approach to Special Care in Dentistry»
Представляем Вашему вниманию похожие книги на «A Practical Approach to Special Care in Dentistry» списком для выбора. Мы отобрали схожую по названию и смыслу литературу в надежде предоставить читателям больше вариантов отыскать новые, интересные, ещё непрочитанные произведения.







Обсуждение, отзывы о книге «A Practical Approach to Special Care in Dentistry» и просто собственные мнения читателей. Оставьте ваши комментарии, напишите, что Вы думаете о произведении, его смысле или главных героях. Укажите что конкретно понравилось, а что нет, и почему Вы так считаете.