John III Beumer - Fundamentals of Implant Dentistry
Здесь есть возможность читать онлайн «John III Beumer - Fundamentals of Implant Dentistry» — ознакомительный отрывок электронной книги совершенно бесплатно, а после прочтения отрывка купить полную версию. В некоторых случаях можно слушать аудио, скачать через торрент в формате fb2 и присутствует краткое содержание. Жанр: unrecognised, на английском языке. Описание произведения, (предисловие) а так же отзывы посетителей доступны на портале библиотеки ЛибКат.
- Название:Fundamentals of Implant Dentistry
- Автор:
- Жанр:
- Год:неизвестен
- ISBN:нет данных
- Рейтинг книги:5 / 5. Голосов: 1
-
Избранное:Добавить в избранное
- Отзывы:
-
Ваша оценка:
Fundamentals of Implant Dentistry: краткое содержание, описание и аннотация
Предлагаем к чтению аннотацию, описание, краткое содержание или предисловие (зависит от того, что написал сам автор книги «Fundamentals of Implant Dentistry»). Если вы не нашли необходимую информацию о книге — напишите в комментариях, мы постараемся отыскать её.
Fundamentals of Implant Dentistry — читать онлайн ознакомительный отрывок
Ниже представлен текст книги, разбитый по страницам. Система сохранения места последней прочитанной страницы, позволяет с удобством читать онлайн бесплатно книгу «Fundamentals of Implant Dentistry», без необходимости каждый раз заново искать на чём Вы остановились. Поставьте закладку, и сможете в любой момент перейти на страницу, на которой закончили чтение.
Интервал:
Закладка:
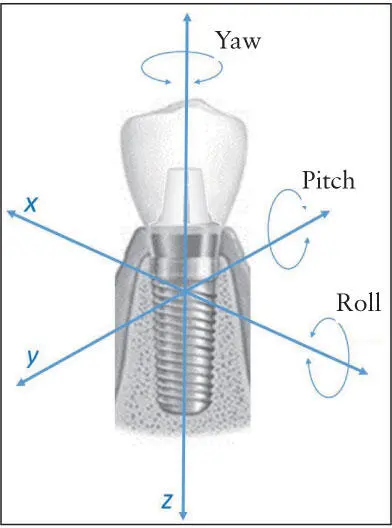
Fig 3-1 Six degrees of freedom that an implant restoration can undergo in response to intraoral forces. The center of mass is the point of lowest resistance to motion at the intersection of the three principal axes.
The three translational forces that act directly on a point tend to produce movement and deformation. Movement can be linear if the force vector acts on the object’s center of mass, resulting in rotation-free bodily movement parallel to the force vector. These forces also produce pure compression/tension on the objects. All other force vectors produce nonaxial movements that involve rotation along with translation. Pure movement happens only in the rare occurrence where an axial force vector is oriented concentrically with the normal axis that lies through the center of mass. By definition, the normal axis is the orthogonal axis that lies perpendicular to the surface. For implants supported by healthy bone, a combination of both translation and compression results. When a vertical force acts on the central axis of an integrated implant, the apical movement (translation) is accompanied by deformation (compression) of the implant and the bone apical to the implant.
Most intraoral forces produce a combination of axial and nonaxial strain components that produce bending, tipping, and rotation around a point of minimum moment of inertia that offers the lowest resistance to each specific motion. By definition, the moment of inertia —or more precisely, the second moment of inertia, also termed the area moment of inertia —is a geometric factor that determines how the 3D shape of an object affects the resistance to deformation such as bending. For maximal resistance (ie, the maximum second moment of inertia), it is desirable to maximize the fractional area to be as far away from the center of mass (more on centroidal axis later in the chapter) as possible. During mastication and oral function, teeth contact and slide over each other by 1.4 to 2.6 mm depending on the type of food and occlusal arrangement. 4The net effect of the applied biting force on each point depends uniquely on the magnitude and direction of the force as well as the distance between the vector and the point. That same force also exerts influence on points that are not aligned along the force axis. The resultant nonaxial force produces rotation and translation of movable objects, bending and shearing of immovable objects, and a combination of both during mastication ( Fig 3-2). This is the reason narrow occlusal tables (see section entitled “Occlusal design for partially edentulous patients”) are beneficial by decreasing the length of the moment arm. As another example, occlusal contact on a cantilever pontic causes axial compression on the pontic material directly below the contact point and causes nonaxial bending at the connector between the pontic and abutment. Because multiple points contact during mastication, the sum of all resolved vectors determines the orientation and net magnitude of deformation or movement.
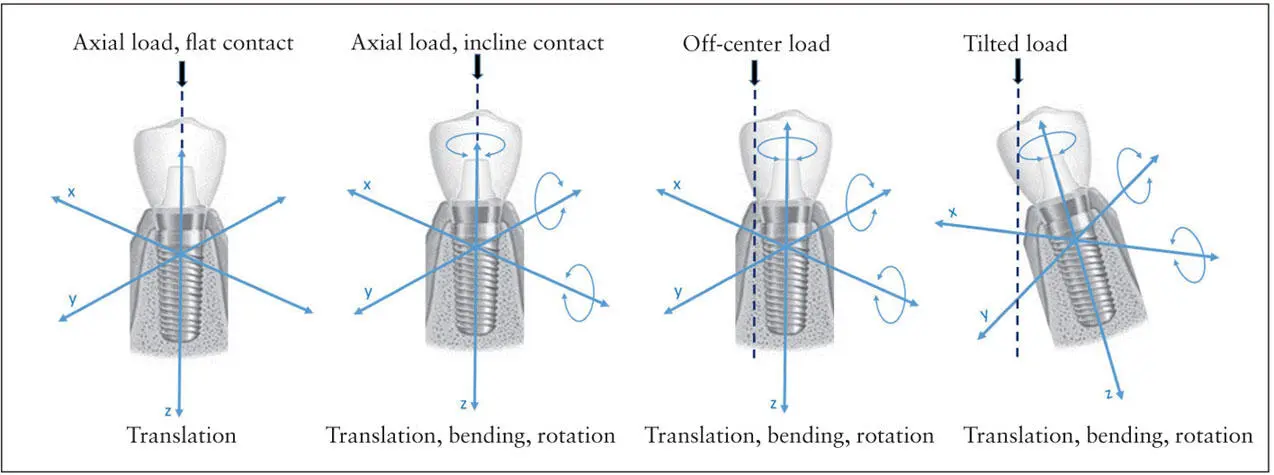
Fig 3-2 Purely axial forces produce pure translation when the contact planes are perpendicular to the load vector. In all other loading scenarios, nonaxial forces are introduced, adding bending and rotation to the deformation.
Nonaxial forces are usually not aligned to take advantage of the resistance offered by the supporting bone, and most materials are weaker in shear than in compression. Therefore, the reduction of excessive nonaxial forces should be a key design rule if long-term stability is a goal of prosthodontic therapy. At the single-tooth level, wide occlusal tables with steep cuspal inclines pose a greater risk of inducing moments throughout the 3D Posselt envelope of motion and should be avoided when the implant support is suboptimal and whenever the expected loads are high (eg, short or narrow implant in compromised bone).
During function, the implant will experience axial and nonaxial loads simultaneously. Several observations have confirmed the favorable effect of axial forces in distributing the stresses evenly within the peri-implant bone. 5– 7Axial loading occurs during closure of the mouth at maximal intercuspation. This is further enhanced if the opposing cusp is occluding against a flat surface, as the applied loads will be parallel to the long axis of the implant. Eventually, the implant and the surrounding bone will be under compression. On the other hand, nonaxial forces will subject the implant to bending moments. These forces can be caused by lateral or oblique application of loads on an implant prosthesis that may occur in situations of occlusal discrepancies, excursive occlusal contacts, bruxism and parafunctional activities, cantilever loading, or occlusal contact on inclined surfaces. 8, 9As a result, the nonaxial forces tend to accentuate the stresses within the bone, prosthesis, and implant components along directions that offer the weakest resistance. This was historically referred to as load magnification and can result in detrimental biologic and mechanical complications. 5, 6, 10
Osseointegrated implants are considerably different from natural teeth biomechanically. Natural teeth are attached to the alveolar bone via the periodontal ligament (PDL), which absorbs and efficiently distributes forces applied on the tooth to the surrounding alveolar bone. In addition, the PDL provides proprioception abilities and maintains some degree of physiologic mobility of the natural teeth. 7, 11, 12As a result, the natural tooth is less vulnerable to suffering from occlusal overloading and can withstand excursive contacts. In comparison, a dental implant is unique in being rigidly connected to bone, so any applied force on the implant prosthesis is directly transferred to the bone. This may lead to excessive stresses and deformation of the surrounding bone, and because the implant is not surrounded by a PDL, there is a reduction of proprioception and mobility. Instead, proprioception and movement of the implant can occur by deformation of bone. In contrast, physiologic mastication results in compression of the natural teeth within their sockets. Therefore, when implants are restored adjacent to natural teeth, the occlusion should allow the natural teeth to compress slightly to allow the implant and natural teeth to distribute the loads evenly. Consequently, the implant and its prosthesis can be subjected to excessive loading, and this overloading can manifest clinically in the form of alveolar bone loss 10and mechanical complications, such as ceramic chipping, screw loosening, material fatigue, creep, and component fracture. 5, 6, 12
The following sections describe the biomechanics of each critical component within the implant-prosthesis system, starting from the dental occlusal design at the most coronal level, down to the prosthetic substructure, the abutment, the implant, and then finally the bone. The important design parameters for each component that influence long-term clinical success are highlighted.
Biomechanics of occlusal design
Numerous case reports, articles, and textbooks have described the importance of dental occlusion when restoring implants. With digital planning using implant component libraries, ideal occlusal schemes can now be designed and executed much more predictably. Planning the appropriate occlusion is important for controlling the load on implant prosthesis-bone systems. Otherwise, occlusal discrepancies predispose to loosening and premature fracture of abutment and prosthetic screws. Besides patient comfort, occlusal discrepancies affect the stability and mobility of implant-assisted overdentures, accelerating wear of attachments and implant connecting bars. Excessive bending moments may also cause micro- fractures within the bone-anchoring implants, triggering a resorptive remodeling response of the anchoring bone and eventual bone loss and implant loss. Occlusal overloading may also have a profound impact on the success or failure of immediately loaded provisional prostheses. Various occlusal schemes and philosophies, whether they were originally developed for complete dentures or fixed prosthodontics, are currently being employed for dental implants depending on the system design.
Читать дальшеИнтервал:
Закладка:
Похожие книги на «Fundamentals of Implant Dentistry»
Представляем Вашему вниманию похожие книги на «Fundamentals of Implant Dentistry» списком для выбора. Мы отобрали схожую по названию и смыслу литературу в надежде предоставить читателям больше вариантов отыскать новые, интересные, ещё непрочитанные произведения.







Обсуждение, отзывы о книге «Fundamentals of Implant Dentistry» и просто собственные мнения читателей. Оставьте ваши комментарии, напишите, что Вы думаете о произведении, его смысле или главных героях. Укажите что конкретно понравилось, а что нет, и почему Вы так считаете.