Paul M. Speight - Shear's Cysts of the Oral and Maxillofacial Regions
Здесь есть возможность читать онлайн «Paul M. Speight - Shear's Cysts of the Oral and Maxillofacial Regions» — ознакомительный отрывок электронной книги совершенно бесплатно, а после прочтения отрывка купить полную версию. В некоторых случаях можно слушать аудио, скачать через торрент в формате fb2 и присутствует краткое содержание. Жанр: unrecognised, на английском языке. Описание произведения, (предисловие) а так же отзывы посетителей доступны на портале библиотеки ЛибКат.
- Название:Shear's Cysts of the Oral and Maxillofacial Regions
- Автор:
- Жанр:
- Год:неизвестен
- ISBN:нет данных
- Рейтинг книги:5 / 5. Голосов: 1
-
Избранное:Добавить в избранное
- Отзывы:
-
Ваша оценка:
Shear's Cysts of the Oral and Maxillofacial Regions: краткое содержание, описание и аннотация
Предлагаем к чтению аннотацию, описание, краткое содержание или предисловие (зависит от того, что написал сам автор книги «Shear's Cysts of the Oral and Maxillofacial Regions»). Если вы не нашли необходимую информацию о книге — напишите в комментариях, мы постараемся отыскать её.
Shear’s Cysts of the Oral and Maxillofacial Regions
Shear’s Cysts of the Oral and Maxillofacial Regions Fifth Edition
Shear's Cysts of the Oral and Maxillofacial Regions — читать онлайн ознакомительный отрывок
Ниже представлен текст книги, разбитый по страницам. Система сохранения места последней прочитанной страницы, позволяет с удобством читать онлайн бесплатно книгу «Shear's Cysts of the Oral and Maxillofacial Regions», без необходимости каждый раз заново искать на чём Вы остановились. Поставьте закладку, и сможете в любой момент перейти на страницу, на которой закончили чтение.
Интервал:
Закладка:
In the first instance, the site of the cyst in the jaws can suggest an initial diagnosis. Odontogenic cysts arise in the tooth‐bearing areas of the jaws in the alveolar bone and in the mandible are always situated above the inferior dental (ID) canal ( Figure 2.1). The cyst displaces the ID canal downwards towards, and sometimes beyond, the lower border of the mandible. Examples of this feature can be seen in Figures 5.5, 5.11 (dentigerous cyst), 7.6, 7.7 (odontogenic keratocyst), 10.4 (glandular odontogenic cyst), 11.3 (calcifying odontogenic cyst), 12.2, and 12.3 (orthokeratinised odontogenic cyst). A cystic radiolucency located below the ID canal is not an odontogenic cyst and when such a feature is seen, an alternative diagnosis must be considered. Figure 17.5 shows a Stafne bone cavity presenting as a radiolucency below the ID canal, excluding the possibility of an odontogenic origin. In the posterior region of the mandible, this judgement is easy to make ( Figure 2.1), but in the anterior mandible and in the maxilla, the distinction between alveolar bone and basal bone is less clear. Although radiolucencies below the ID canal cannot be odontogenic, the converse is not true and a number of radiolucent lesions of non‐odontogenic origin may arise above the ID canal. Figure 17.1 shows an example of a simple bone cyst that is not odontogenic, but characteristically lies within the alveolar bone and embraces the roots of multiple teeth. Other lesions that may arise in the alveolar bone and be associated with tooth roots include giant cell granuloma, Langerhans cell histiocytosis, and ossifying fibroma. Non‐cystic odontogenic lesions, including periapical granulomas, odontogenic tumours, cemento‐osseous dysplasias, and cementoblastoma, must also be considered in the differential diagnosis of lesions in the tooth‐bearing area. Overall, however, odontogenic cysts and in particular radicular cysts are by far the most common.
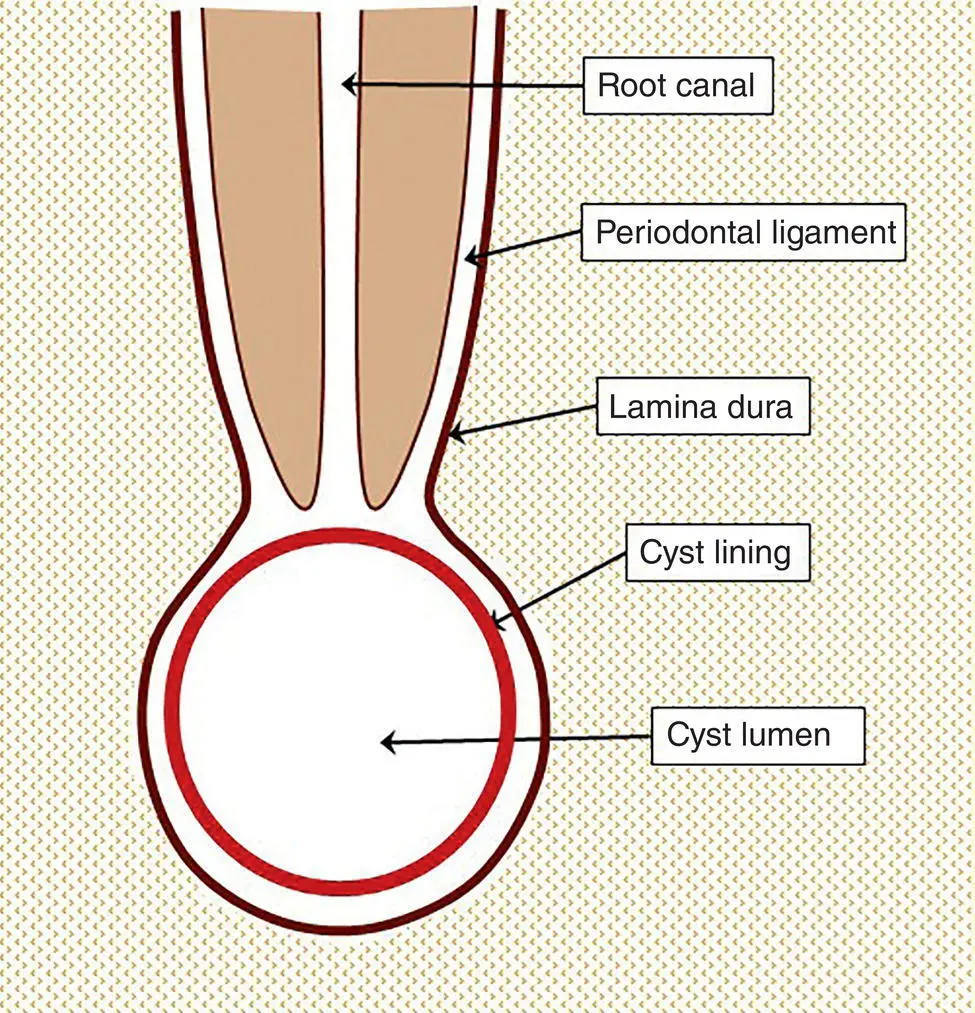
Figure 2.2 Diagrammatic representation of a radicular cyst. The cyst develops from rest cells of Malassez within the periodontal ligament, and lies within the lamina dura. The corticated margin of the cyst is continuous with the lamina dura (see text for details).
The defining feature of the radicular cyst is of a radiolucency associated with the apex of a non‐vital tooth ( Table 2.2; Figure 3.4). The radicular cyst arises within the periodontal ligament from the rest cells of Malassez, and an important sign is that the cyst lies within the lamina dura that surrounds the root of the tooth. Furthermore, the corticated margin of the cyst is continuous with the lamina dura ( Figure 2.2). Although this feature is helpful in diagnosing a radicular cyst, it is of more value in excluding a radicular cyst when another cyst type appears to be associated with a tooth root. If a cystic radiolucency is associated with the root of a tooth, but the lamina dura is intact, then a radicular cyst can be excluded and another diagnosis must be considered. This feature is especially helpful in the diagnosis of inflammatory collateral cysts ( Figures 4.2and 4.3), lateral periodontal cyst (Figure 8.2), nasopalatine duct cyst (Figures 13.7 and 13.8), surgical ciliated cyst (Figure 16.2), and simple bone cyst (Figure 17.1).
It must be noted, however, that other lesions arise within the periodontal ligament and may lie within the lamina dura. In particular, a periapical granuloma may have an identical radiological appearance to a radicular cyst, and it is not possible to reliably distinguish between a granuloma and a cyst (discussed in detail in Chapter 3). Although cysts are often larger (see Table 3.1), when a radiolucency is encountered at the apex of a tooth there is an equal chance that the lesion is a periapical granuloma or a radicular cyst (Jones and Franklin 2006a ,b ; Koivisto et al. 2012 ; discussed in Chapter 1). Cemental lesions also arise within the periodontal ligament and, especially when small and not fully calcified, may present as a radiolucency identical to radicular cyst. This feature may be seen in lesions of cemento‐osseous dysplasia, cemento‐ossifying fibroma, and cementoblastoma. The dentigerous cyst embraces the crown of an unerupted tooth and cannot be confused with radicular cyst, but the corticated margin is continuous with the lamina dura (Figures 5.5 and 5.6).
Histopathological Examination of Cysts
In most cases the responsibility for a final diagnosis lies with the histopathologist who must examine samples of tissue. As stated above, it is important that the pathologist does not make a final diagnosis without first considering the clinical and radiological features of the lesion. These may be stated on the pathology request form, but often the pathologist should read the radiology report, consult with the radiologist, or personally examine the radiographs. Many cysts may reach a large size and it is good practice to establish a diagnosis before definitive surgery. This means that the histopathologist is often presented with a small incisional biopsy of a large lesion. In most cases, consideration of the radiological and histological features together is sufficient to establish a diagnosis. The key features summarised in Tables 2.2and 2.3should assist decision making in most cases. Occasionally a definitive diagnosis is not possible on a small biopsy and a final diagnosis must await examination of the whole specimen. Pathologists must not be afraid to withhold a final diagnosis until it has been possible to examine sufficient tissue.
Histopathological examination of a cyst begins with examination and sampling of the whole specimen. If an associated tooth is also removed, then the relationship of the cyst to the tooth can be directly observed and is of particular value in the diagnosis of a radicular cyst (located at the tooth apex), dentigerous cyst (attached at the cementoenamel junction; Figure 5.18), and paradental cyst (attached to the disto‐buccal aspect of the tooth; Figure 4.6). In all cases it is of value to examine the cyst in its entirety and also to dissect it and examine the cut surface and the lumen. Most cysts are unilocular with a thin regular lining, but careful examination of the gross specimen will show evidence of multilocularity and reveal areas of thickening or luminal nodules if present. Cysts that are typically multilocular on gross examination include the botryoid odontogenic cyst (Figures 8.3, 8.9, and 8.10) and glandular odontogenic cyst (Figure 10.6). Thickening of the wall or luminal nodules are seen in lateral periodontal cyst (Figure 8.6), glandular odontogenic cyst (Figures 10.6 and 10.8), and calcifying odontogenic cyst (Figures 11.8 and 11.9). Calcifying odontogenic cyst may also have calcified material in the wall or be associated with an odontoma. Representative samples of the cyst wall, including any areas of thickening, should be taken for histological examination and any hard tissue should be decalcified and sampled for histology.
On dissection, most cysts contain small amounts of serosanguinous fluid, but the odontogenic keratocyst and orthokeratinised odontogenic cyst usually contain a ‘cheesy’ or ‘buttery’ keratinaceous material that is cream or yellow coloured, and may have a characteristically unpleasant odour. Such contents will be familiar to many pathologists as a characteristic feature of epidermal cysts of the skin.
The histological features of each cyst and the histological differential diagnosis are described in detail in each chapter. Very few cysts have histological features that are absolutely diagnostic or pathognomonic, and diagnosis is usually made by considering a combination of features in the context of the radiology. The only possible exception to this is the odontogenic keratocyst, which shows a thin regular lining of parakeratinised epithelium with features that are unique to this cyst type (see Figures 7.15–7.17). Table 2.3provides an overview of characteristic histological features and their diagnostic utility for different cyst types.
Читать дальшеИнтервал:
Закладка:
Похожие книги на «Shear's Cysts of the Oral and Maxillofacial Regions»
Представляем Вашему вниманию похожие книги на «Shear's Cysts of the Oral and Maxillofacial Regions» списком для выбора. Мы отобрали схожую по названию и смыслу литературу в надежде предоставить читателям больше вариантов отыскать новые, интересные, ещё непрочитанные произведения.


Обсуждение, отзывы о книге «Shear's Cysts of the Oral and Maxillofacial Regions» и просто собственные мнения читателей. Оставьте ваши комментарии, напишите, что Вы думаете о произведении, его смысле или главных героях. Укажите что конкретно понравилось, а что нет, и почему Вы так считаете.