Ceri Davies - Textbook for Orthodontic Therapists
Здесь есть возможность читать онлайн «Ceri Davies - Textbook for Orthodontic Therapists» — ознакомительный отрывок электронной книги совершенно бесплатно, а после прочтения отрывка купить полную версию. В некоторых случаях можно слушать аудио, скачать через торрент в формате fb2 и присутствует краткое содержание. Жанр: unrecognised, на английском языке. Описание произведения, (предисловие) а так же отзывы посетителей доступны на портале библиотеки ЛибКат.

- Название:Textbook for Orthodontic Therapists
- Автор:
- Жанр:
- Год:неизвестен
- ISBN:нет данных
- Рейтинг книги:4 / 5. Голосов: 1
-
Избранное:Добавить в избранное
- Отзывы:
-
Ваша оценка:
Textbook for Orthodontic Therapists: краткое содержание, описание и аннотация
Предлагаем к чтению аннотацию, описание, краткое содержание или предисловие (зависит от того, что написал сам автор книги «Textbook for Orthodontic Therapists»). Если вы не нашли необходимую информацию о книге — напишите в комментариях, мы постараемся отыскать её.
Written to help the reader understand the role and function of an orthodontic therapist,
offers support to those undertaking the Diploma in Orthodontic Therapy and to assist those who already work as orthodontic therapists, helping them in their quest to enhance safe and effective care.
Textbook for Orthodontic Therapists — читать онлайн ознакомительный отрывок
Ниже представлен текст книги, разбитый по страницам. Система сохранения места последней прочитанной страницы, позволяет с удобством читать онлайн бесплатно книгу «Textbook for Orthodontic Therapists», без необходимости каждый раз заново искать на чём Вы остановились. Поставьте закладку, и сможете в любой момент перейти на страницу, на которой закончили чтение.
Интервал:
Закладка:
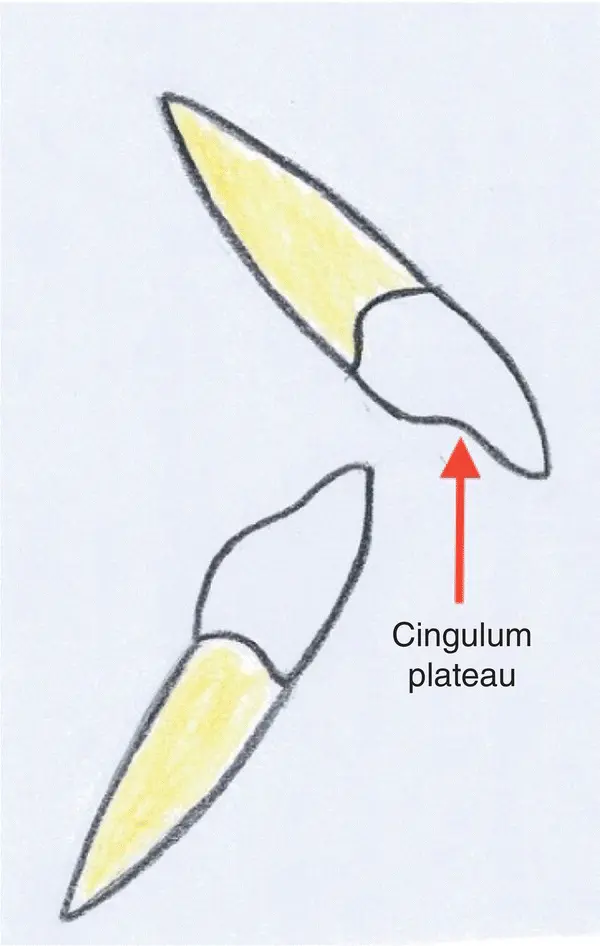
Figure 3.5 Incisor relationship class II div I.
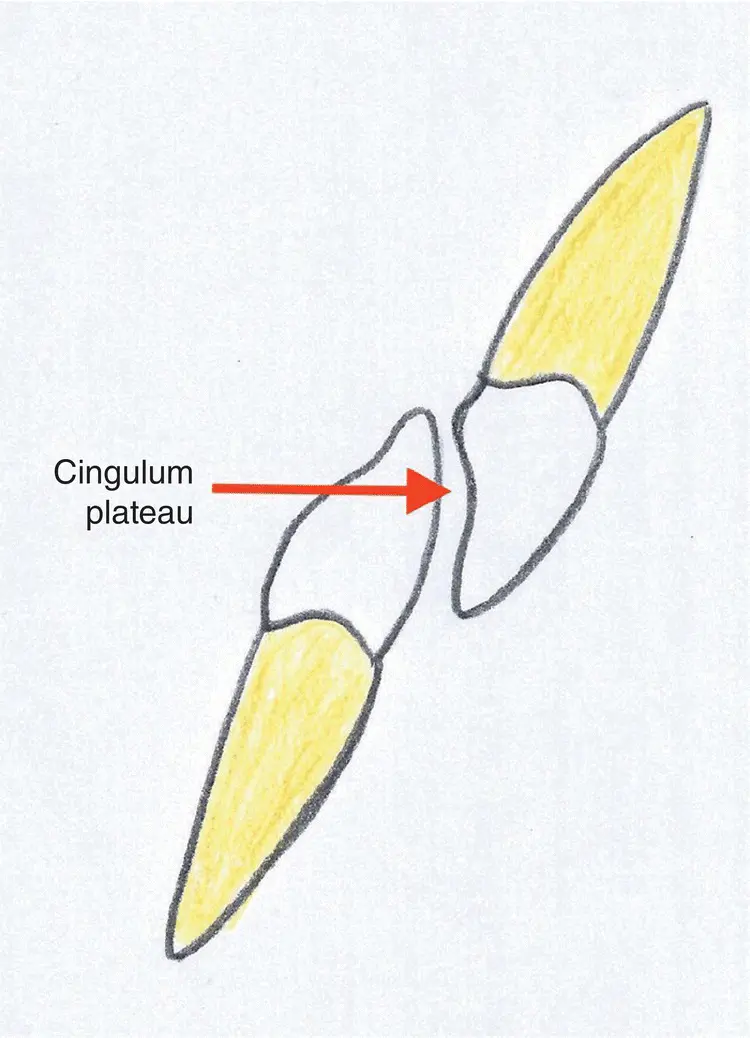
Figure 3.6 Incisor relationship class II div II.
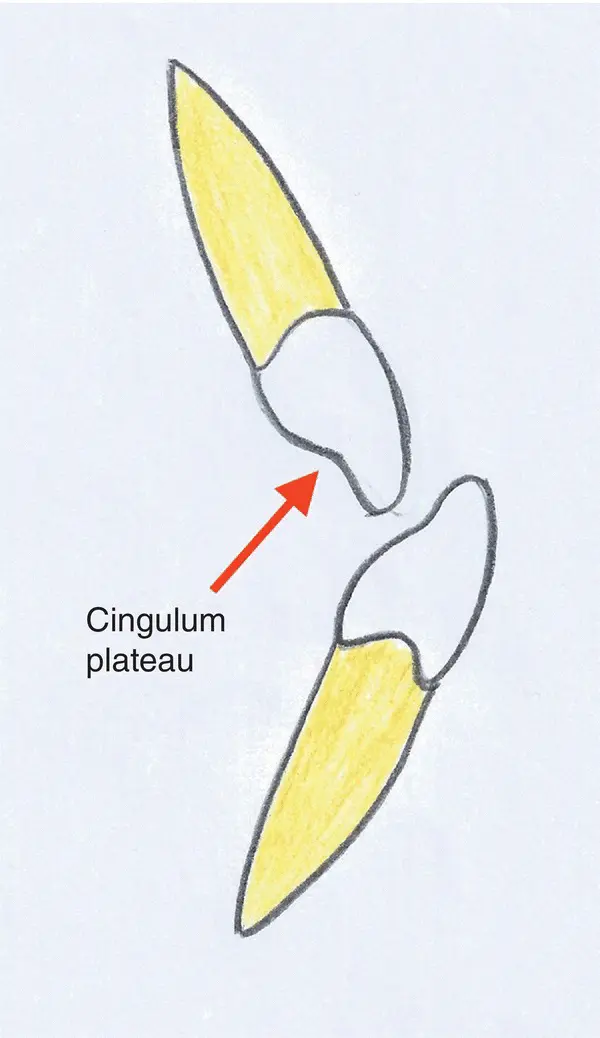
Figure 3.7 Incisor relationship class III.
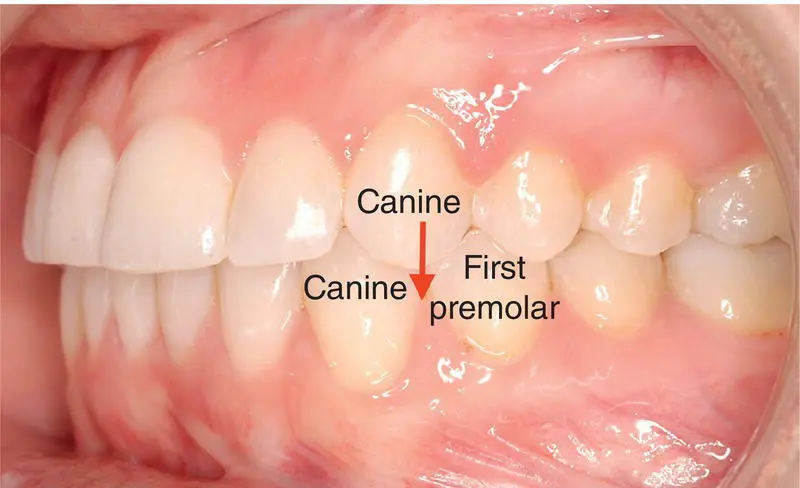
Figure 3.8 Class I canine relationship.
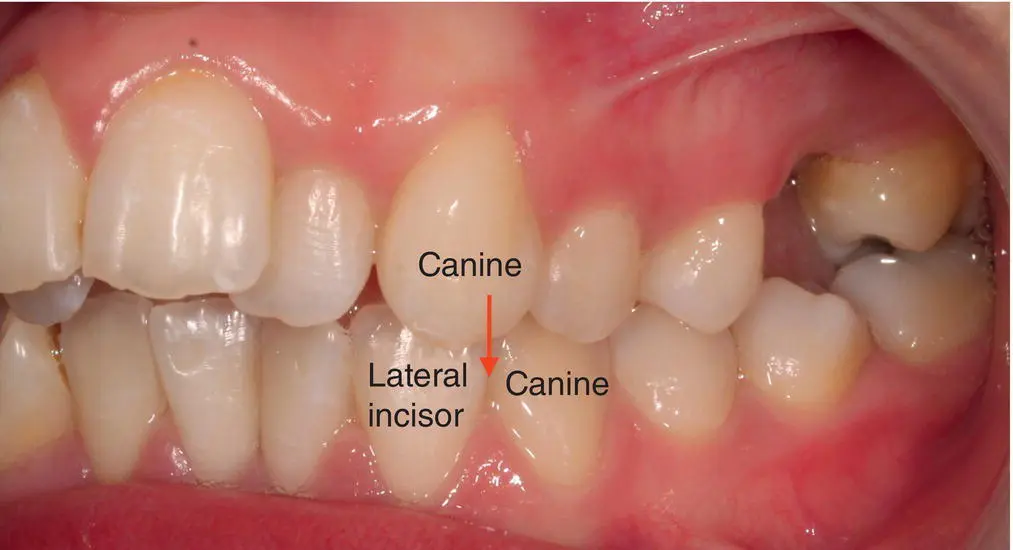
Figure 3.9 Class II canine relationship.

Figure 3.10 Class III canine relationship.
3.4 Andrew’s Six Keys
This classification was developed by Lawrence Andrews, the same orthodontist who developed the preadjusted edgewise appliance. Over time Andrews decided that it was not always possible to achieve a good class I occlusion, therefore the six keys were developed to identify each feature to evaluate why this was not possible. A seventh key was added subsequently because correct tooth size can have an effect on achieving good class I occlusion.
1 Correct molar relationship:The mesiobuccal cusp of the upper first molar occludes in the buccal groove of the lower first molar.The distobuccal cusp of the upper first molar occludes on the mesiobuccal cusp of the lower second molar.
2 Correct crown angulation:All tooth crowns are angulated mesially.
3 Correct crown inclination:Incisors are inclined towards the buccal or labial surface.Buccal segment teeth are inclined lingually; in the lower buccal segments this is progressive.
4 Flat curve of Spee.
5 No rotations.
6 No spaces.
7 Correct tooth size.
4 Aetiology of Malocclusion
This chapter will look at all the different types of causes for the types of malocclusions we see in orthodontics.
4.1 Skeletal Factors
Skeletal factors are categorised into all three planes of space.
4.1.1 Anteroposterior Plane (AP)
Dento‐alveolar compensation is a term used when teeth compensate for the skeletal pattern. For example, a patient may have class I incisors but be presenting with a class III skeletal pattern.
4.1.2 Vertical Plane
Growth rotations occur in the mandible. This is extra growth which can be seen once the patient has stopped growing. There are two types:
Forward growth rotation – decreased lower anterior facial height (LAFH).
Backward growth rotation – increased LAFH.
4.1.3 Transverse Plane
Absolute transverse maxillary deficiency:
This term relates to crossbites and is most commonly seen in class III cases.
Commonly seen in maxillary retrusion, this is where the maxilla is reduced in all three dimensions, which can result in crossbites anteriorly and posteriorly.
Dento‐alveolar compensation:
This term is used when teeth compensate for the skeletal pattern.
In this case transversely, teeth can compensate to result in a crossbite being present.
For example, tipping of the buccal surface of the upper molar and lingual surface of the lower molar compensates for transverse maxillary deficiency.
4.2 Soft Tissue Factors
4.2.1 Fullness and Tone of the Lips
The fullness and tone of lips can have an effect on the dentition, as they can result in positioning of the incisors in the labiolingual direction. The effects can include the following:
Lips that lack muscular tone and are flaccid – incisors tend to be proclined.
Strap‐like lips:Lips are tense and the incisors tend to be retroclined.The term highly active lip can also be used to describe this.
Lower lip line:The lower lip should cover one‐third to one‐half of the upper incisor crowns.More than one‐half coverage = retroclined upper incisors.Less than one‐third coverage = proclined upper incisors.
4.2.2 Lip Competency
Lip competency looks at how the lips are when the patient is at rest. There are two types of lip competency:
Competent lips, which is where minimal effort is required to achieve an oral seal.
Incompetent lips, which is where excessive muscular activity is required to achieve an oral seal.
With incompetent lips the following features can be found:Can often be associated with a low lower lip line.Swallowing patterns may occur to achieve an anterior oral seal. If excessive muscular activity or forward mandibular posturing is not possible to achieve, then the following swallowing patterns can occur:Tongue to lower lip results in incisor proclination.Lower lip to palate results in upper incisor proclination and lower incisor retroclination.Tongue to upper lip results in upper incisor proclination.
4.2.3 Macroglossia (Large Tongue)
The size of the tongue can affect the development of the dentition. The tongue can also impede incisor eruption and anterior open bite (AOB). The tongue can present with two types of tongue thrusts:
Adaptive tongue thrust: this can be corrected and stopped once the positions of the teeth are corrected. It is seen when the tongue is forced between the teeth.
Endogenous tongue thrust: this is where the tongue is thrusted forward between the teeth, but is a habit that may not be stopped once tooth positions have been corrected. This can result in relapse.
4.2.4 Enlarged Adenoids
Adenoids are large glands which are located by the soft palate in the roof of the mouth. Enlarged adenoids can result in the development of an AOB due to constant mouth breathing. This has the effect of the molars over‐erupting and resulting in an increased LAFH.
4.2.5 Generalised Pathology of Muscles
Muscle weakness can also have an effect on the dentition. Weak muscles enable the teeth to move due to the lack of support of the soft tissues surrounding the dentition.
4.3 Local Factors
Local factors are divided into three groups:
Variation in tooth number
Variation in tooth size
Variation in tooth position.
4.3.1 Variation in Tooth Number
4.3.1.1 Hypodontia
Hypodontia is known as missing teeth.
Hypodontia is found when there is an absence of one or more primary or secondary teeth, excluding third molars.
The most common cause can be genetic, with a family history of hypodontia.
The most common missing teeth are upper third molars (U8s), lower third molars (L8s), lower premolars (L5s), upper lateral incisors (U2s), upper premolars (U5s), and lower central incisors (L1s).
4.3.1.2 Supernumerary
Supernumerary teeth are extra teeth.
Supernumerary teeth are found when there are excessive teeth in the normal series.
Читать дальшеИнтервал:
Закладка:
Похожие книги на «Textbook for Orthodontic Therapists»
Представляем Вашему вниманию похожие книги на «Textbook for Orthodontic Therapists» списком для выбора. Мы отобрали схожую по названию и смыслу литературу в надежде предоставить читателям больше вариантов отыскать новые, интересные, ещё непрочитанные произведения.





Обсуждение, отзывы о книге «Textbook for Orthodontic Therapists» и просто собственные мнения читателей. Оставьте ваши комментарии, напишите, что Вы думаете о произведении, его смысле или главных героях. Укажите что конкретно понравилось, а что нет, и почему Вы так считаете.