Protocols for High-Risk Pregnancies
Здесь есть возможность читать онлайн «Protocols for High-Risk Pregnancies» — ознакомительный отрывок электронной книги совершенно бесплатно, а после прочтения отрывка купить полную версию. В некоторых случаях можно слушать аудио, скачать через торрент в формате fb2 и присутствует краткое содержание. Жанр: unrecognised, на английском языке. Описание произведения, (предисловие) а так же отзывы посетителей доступны на портале библиотеки ЛибКат.

- Название:Protocols for High-Risk Pregnancies
- Автор:
- Жанр:
- Год:неизвестен
- ISBN:нет данных
- Рейтинг книги:3 / 5. Голосов: 1
-
Избранное:Добавить в избранное
- Отзывы:
-
Ваша оценка:
Protocols for High-Risk Pregnancies: краткое содержание, описание и аннотация
Предлагаем к чтению аннотацию, описание, краткое содержание или предисловие (зависит от того, что написал сам автор книги «Protocols for High-Risk Pregnancies»). Если вы не нашли необходимую информацию о книге — напишите в комментариях, мы постараемся отыскать её.
has helped busy obstetricians keep pace with a constantly evolving field. Providing just-in-time content, its focus on protocols and guidelines helps organize medical thinking, avoid heuristic errors of omission and commission, and optimize maternal and fetal outcomes.
As with the prior six editions, the editors have once again assembled some of the world’s top obstetrical and medical experts. This seventh edition has also been expanded to include a number of new topics, including:
Protocols on opioid use, misuse and addition in pregnancy and postpartum Noninvasive prenatal diagnosis of aneuploidy Periconceptual genetic screening Expanded protocols on maternal valvular heart disease and cardiomyopathies Protocols on arboviruses, including Zika and malaria
will be an essential reference for obstetricians, medical students, general practitioners and all medical professionals who are seeking the most up-to-date information and guidance on high-risk pregnancies.
Protocols for High-Risk Pregnancies — читать онлайн ознакомительный отрывок
Ниже представлен текст книги, разбитый по страницам. Система сохранения места последней прочитанной страницы, позволяет с удобством читать онлайн бесплатно книгу «Protocols for High-Risk Pregnancies», без необходимости каждый раз заново искать на чём Вы остановились. Поставьте закладку, и сможете в любой момент перейти на страницу, на которой закончили чтение.
Интервал:
Закладка:
If a diagnosis of folate deficiency is made, or the woman had a prior pregnancy affected by a neural tube defect, the recommended dose of folic acid is 4 mg/day. Anemia due to folate or B 12deficiency should respond briskly, with an elevated reticulocyte count, within 4–7 days of beginning treatment. In the case of macrocytic anemia with normal folate and vitamin B 12levels, a consultation with a hematologist is indicated for bone marrow biopsy.
Normocytic anemia
The recommended laboratory evaluation for normocytic anemia is displayed in Figure 11.2. A high reticulocyte count indicates either hemolysis or blood loss with resultant bone marrow activation. If a normocytic anemia with an elevated reticulocyte count is found, a careful history and evaluation of laboratory studies for hemolysis, such as Coombs test, peripheral smear, and lactate dehydrogenase level, should be undertaken. A normal or low reticulocyte count in the setting of anemia raises concern for iron deficiency (a ferritin level less than 10–15 μg/dL is diagnostic) or bone marrow suppression/disorders. Low reticulocyte count with normal or high serum ferritin levels can be seen in the presence of hypothyroidism or chronic disorders, such as inflammatory bowel disease, systemic lupus erythematosus, granulomatous infections, malignant neoplasms, and rheumatoid arthritis. Hematology consultation for further assessment is indicated in these circumstances.
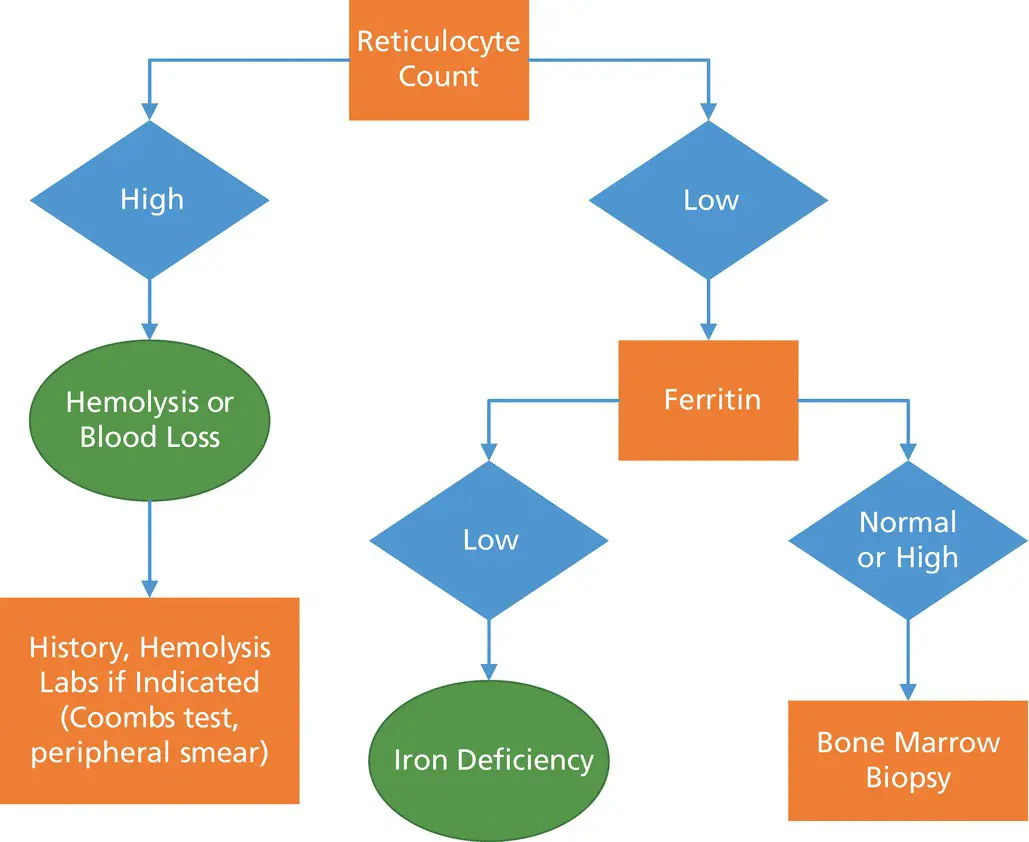
Figure 11.2 Algorithm for evaluation of normocytic anemia.
Mixed nutritional deficiencies (folate and iron) may lead to normocytic anemia in pregnancy, but routine supplementation makes the probability of such a scenario low. If concern for a mixed nutritional deficiency does arise, the red cell distribution width (RDW), a marker of increased variability in red cell size or anisocytosis, is a useful indicator as an RDW greater than 15% indicates the presence of nutritional deficiencies.
Microcytic anemia
Most cases of microcytic anemia in pregnancy are due to iron deficiency anemia. Evaluation of a ferritin level should be the next step, as shown in Figure 11.3. Serum ferritin is the most sensitive and specific screening test for iron deficiency, with a level less than 10–15 μg/dL indicating depleted iron stores. If serum ferritin is normal or high, the next step is hemoglobin electrophoresis to evaluate for a thalassemia. Such situations usually warrant consultation with a hematologist for further evaluation and bone marrow biopsy as indicated.
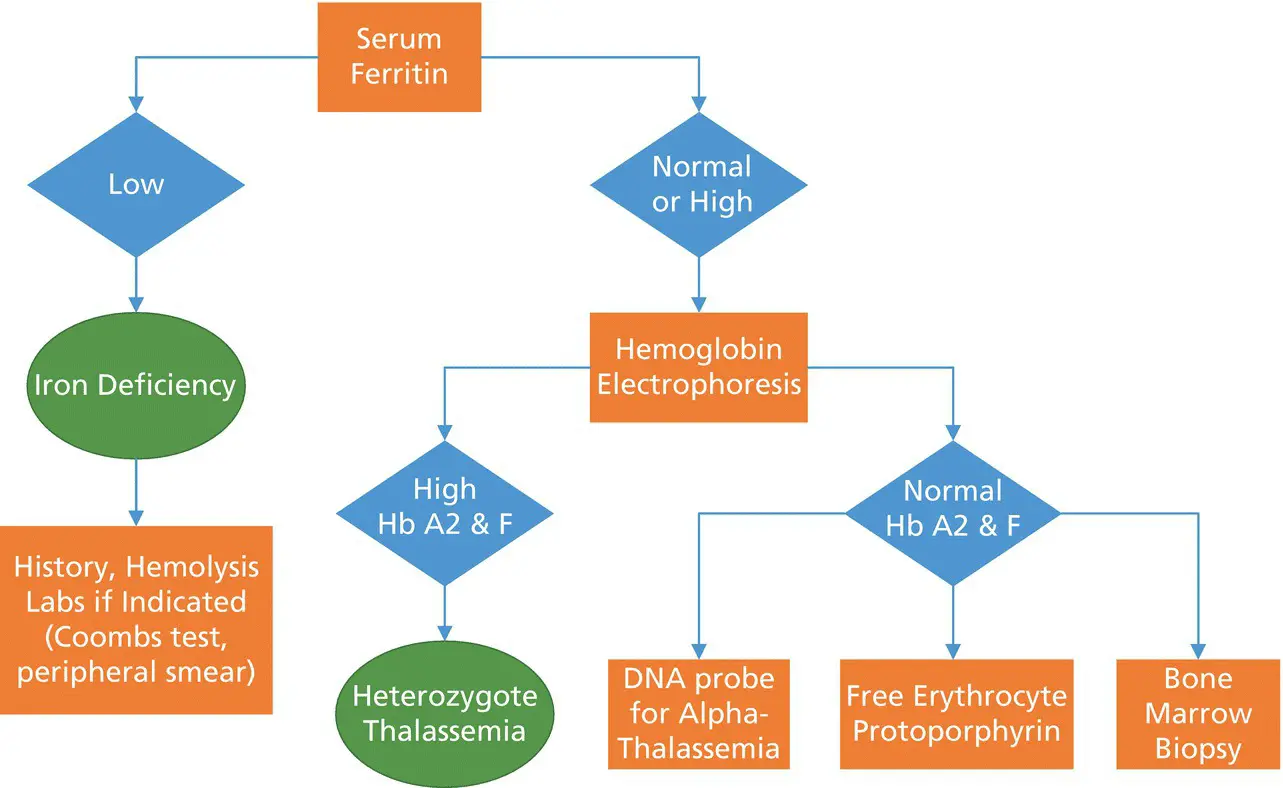
Figure 11.3 Algorithm for evaluation of microcytic anemia.
Iron supplementation in pregnancy
In a typical singleton gestation, maternal iron requirements (including blood volume expansion as well as fetal and placental requirements) average 1 g for the entire pregnancy, with this requirement further increased in the setting of multiple gestations. In a landmark study of healthy, nonanemic, menstruating young women who agreed to bone marrow biopsy, 66% had inadequate iron stores. For the above reasons, and because gastrointestinal side effects of oral iron supplementation (constipation, nausea, and diarrhea) are negligible with doses less than 45–60 mg, supplementation with elemental iron (30 mg/day) is recommended for all pregnant women in the United States, regardless of indices.
Supplementation should be continued until three months postpartum in areas with high prevalence of anemia. A review of randomized clinical trials (most performed in Western countries) showed that routine supplementation in nonanemic women results in higher maternal Hb levels at term and one month postpartum, higher serum ferritin levels, lower rates of anemia at term (RR = 0.26) and of iron deficiency anemia in particular (RR = 0.33), and higher serum ferritin levels in the infants (Peña‐Rosas and Viteri 2009). However, no differences are noted in most clinical outcomes, such as preterm birth, preeclampsia, or need for transfusion, birthweight, small for gestational age, perinatal mortality or need for NICU admissions.
Treatment of iron deficiency anemia
Compared to routine supplementation in pregnancy, higher doses of iron are required for the treatment of maternal anemia (up to 200 mg/day). Oral iron therapy is most often utilized, with a list of the most commonly available formulations given in Table 11.2. Enteric‐coated forms should be avoided because they are poorly absorbed; absorption is increased by intake of iron on an empty stomach and with vitamin C or orange juice. Although several trials have been conducted to compare iron formulations, it is not possible to assess the efficacy of the treatments due to the use of different drugs, doses, and routes. Gut absorption decreases with increasing doses of iron; therefore it is best to divide the total daily dose into 2–3 doses.
Table 11.2 Oral preparations for therapy of iron deficiency anemia
Source: Based on ACOG Practice Bulletin No. 107, 2009.
| Type of iron | Elemental iron (mg) | Brand |
|---|---|---|
| Ferrous fumarate | 64–200 | Femiron, Feostat, Ferrets, Fumasorb, Hemocyte, Ircon, Nephro‐Fer, Vitron‐C |
| Ferrous sulfate | 40–65 | Chem‐Sol, Fe50, Feosol, Fergensol, Ferinsol, Ferogradumet, Ferosul, Ferratab, FerraTD, Ferrobob, Ferrospace, Ferrotime, Moliron, Slowfe, Yieronia |
| Ferrous gluconate | 38 | Fergon, Ferralet, Simron |
| Ferric | 50–150 | Ferrimin, Fe‐Tinic, Hytinic, Niferex, Nu‐iron |
A relationship exists between dose of oral iron and gastrointestinal side effects, with worsening of symptoms as dose increases, with such side effects leading to discontinuation of therapy in 50% of women. To encourage compliance, it is important to minimize side effects by increasing the dose gradually, with larger doses in the evening, and consideration for the use of an iron sulfate elixir which allows more gradual titration of dose. Stool softeners are often required to prevent constipation. Serum reticulocyte count should be elevated within 7–10 days of treatment initiation, with an improvement in hemoglobin levels less rapid – the hemoglobin deficit should be expected to halve in one month and normalize by 6–8 weeks after initiation of treatment. To replenish iron stores, oral therapy should be continued for three months after the anemia has been corrected.
Intravenous (IV) iron therapy is generally reserved for women who cannot or will not take oral iron preparations. Hemoglobin indices are equivalent after 40 days of treatment in women receiving IV iron therapy compared to those receiving oral therapy, but the rate of rise is more rapid in women receiving IV therapy. Randomized trials have not shown significant differences in need for maternal blood transfusion, neonatal birthweight, or neonatal anemia between the two forms of supplementation, and studies have demonstrated a preference for oral supplementation among most women. Therefore, IV therapy is indicated only in patients with severe anemia with intolerance to oral therapy or malabsorption. Iron dextran is associated with a greater risk of anaphylaxis and is not recommended in the light of other available formulations with a lower risk of allergic reaction. Intravenous preparations tested in pregnancy or puerperium are shown in Table 11.3.
Читать дальшеИнтервал:
Закладка:
Похожие книги на «Protocols for High-Risk Pregnancies»
Представляем Вашему вниманию похожие книги на «Protocols for High-Risk Pregnancies» списком для выбора. Мы отобрали схожую по названию и смыслу литературу в надежде предоставить читателям больше вариантов отыскать новые, интересные, ещё непрочитанные произведения.












Обсуждение, отзывы о книге «Protocols for High-Risk Pregnancies» и просто собственные мнения читателей. Оставьте ваши комментарии, напишите, что Вы думаете о произведении, его смысле или главных героях. Укажите что конкретно понравилось, а что нет, и почему Вы так считаете.