Endodontic Materials in Clinical Practice
Здесь есть возможность читать онлайн «Endodontic Materials in Clinical Practice» — ознакомительный отрывок электронной книги совершенно бесплатно, а после прочтения отрывка купить полную версию. В некоторых случаях можно слушать аудио, скачать через торрент в формате fb2 и присутствует краткое содержание. Жанр: unrecognised, на английском языке. Описание произведения, (предисловие) а так же отзывы посетителей доступны на портале библиотеки ЛибКат.
- Название:Endodontic Materials in Clinical Practice
- Автор:
- Жанр:
- Год:неизвестен
- ISBN:нет данных
- Рейтинг книги:4 / 5. Голосов: 1
-
Избранное:Добавить в избранное
- Отзывы:
-
Ваша оценка:
Endodontic Materials in Clinical Practice: краткое содержание, описание и аннотация
Предлагаем к чтению аннотацию, описание, краткое содержание или предисловие (зависит от того, что написал сам автор книги «Endodontic Materials in Clinical Practice»). Если вы не нашли необходимую информацию о книге — напишите в комментариях, мы постараемся отыскать её.
Presents an illustrated guide to all materials used in endodontic practice Focuses on the clinical application for each material Explains why specific materials are used Includes information on how to select the correct material Considers locations and techniques in making material decisions Written for specialist endodontists and residents, dental material specialists, post-graduate students, general dentists, and dentistry students,
is an essential resource for selecting the right materials for specific techniques.
Endodontic Materials in Clinical Practice — читать онлайн ознакомительный отрывок
Ниже представлен текст книги, разбитый по страницам. Система сохранения места последней прочитанной страницы, позволяет с удобством читать онлайн бесплатно книгу «Endodontic Materials in Clinical Practice», без необходимости каждый раз заново искать на чём Вы остановились. Поставьте закладку, и сможете в любой момент перейти на страницу, на которой закончили чтение.
Интервал:
Закладка:
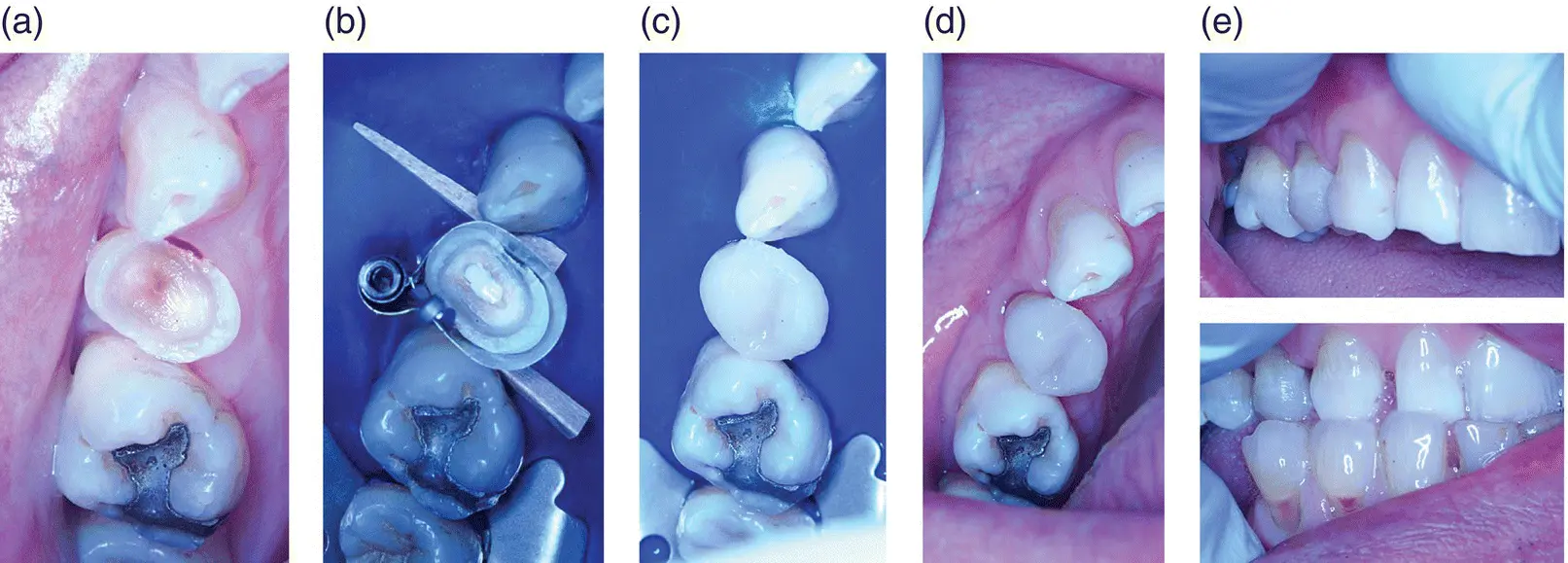
Figure 2.3 Intraoral photographs of an indirect pulp‐capping procedure. (a) Preoperative image of a grossly broken‐down upper right first premolar, showing a deep lesion with unexposed pulp. (b) Indirect pulp cap with a thin layer of Biodentine interfacing with dentine overlying the pulp, leaving the maximum amount of bonding tooth tissue available for a direct composite resin restoration. (c) Direct composite resin build‐up. (d) Occlusal view of completed restoration. (e) Buccal view of composite resin restoration.
Source: Phillip L. Tomson.
2.3.3.1 Direct Pulp Capping
This procedure is carried out if dentine is lost due to caries, trauma, or a previous iatrogenic intervention and a cavity exists where the soft tissue of the pulp is exposed (≤2.5 mm) and (in most cases) bleeding. Direct pulp capping is defined as application of a material directly on to the pulp with the aim of producing a positive biological response so that the pulp can protect itself. This treatment strategy may be applied out if a tooth is symptomless or has relatively mild symptoms ( Figure 2.4).
2.3.3.2 Partial Pulpotomy
This procedure is carried out if dentine is lost due to caries, trauma, or a previous iatrogenic intervention and a cavity exists where the soft tissue of the pulp is exposed and bleeding, suggesting it is inflamed. The amount of bleeding is used as a surrogate marker of inflammation. Partial pulpotomy is defined as removal of a small portion of superficial coronal pulp tissue followed by application of a material directly on to the pulp with the aim of producing a positive biological response so that the pulp can protect itself. With this treatment strategy, pulp tissue is removed approximately 2 mm at a time and then an attempt is made to obtain haemostasis as previously described. If haemostasis is not achieved, the process is repeated ( Figure 2.5).
2.3.3.3 Full Pulpotomy
This procedure is carried out when there is gross loss of dentine due to caries, trauma, or previous iatrogenic intervention and a cavity exists where a large portion of the soft tissue of the pulp is exposed and bleeding, suggesting inflammation or contamination, or where it is not possible to obtain haemostasis at a superficial level. Full pulpotomy is defined as complete removal of the coronal pulp to the root canal orifice level, followed by application of a material directly on to the remaining pulp with the aim of producing a positive biological response so that the pulp can protect itself ( Figure 2.6).
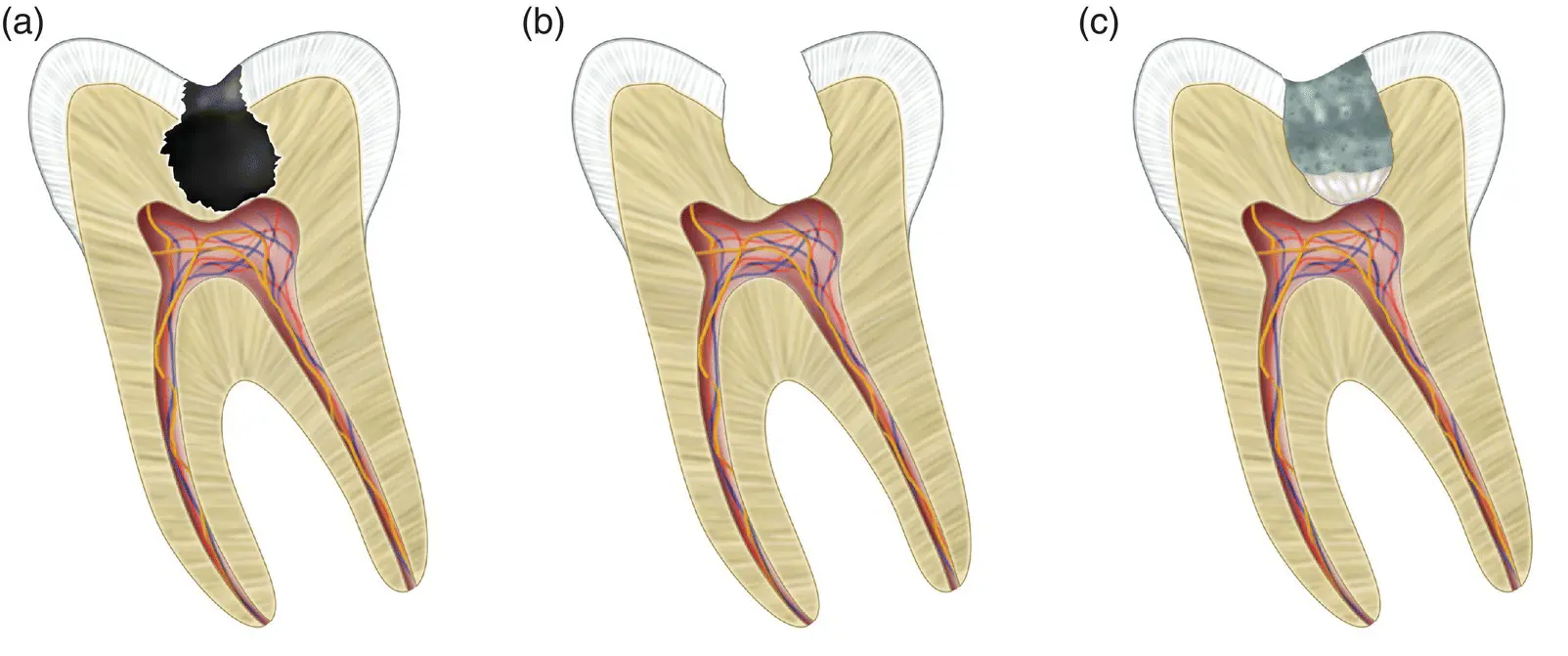
Figure 2.4 Direct pulp capping. (a) Deep carious lesion extending to the pulp. (b) Carious exposure of the pulp following cavity preparation. (c) Calcium silicate cement directly interfacing with the pulp following definitive restoration.
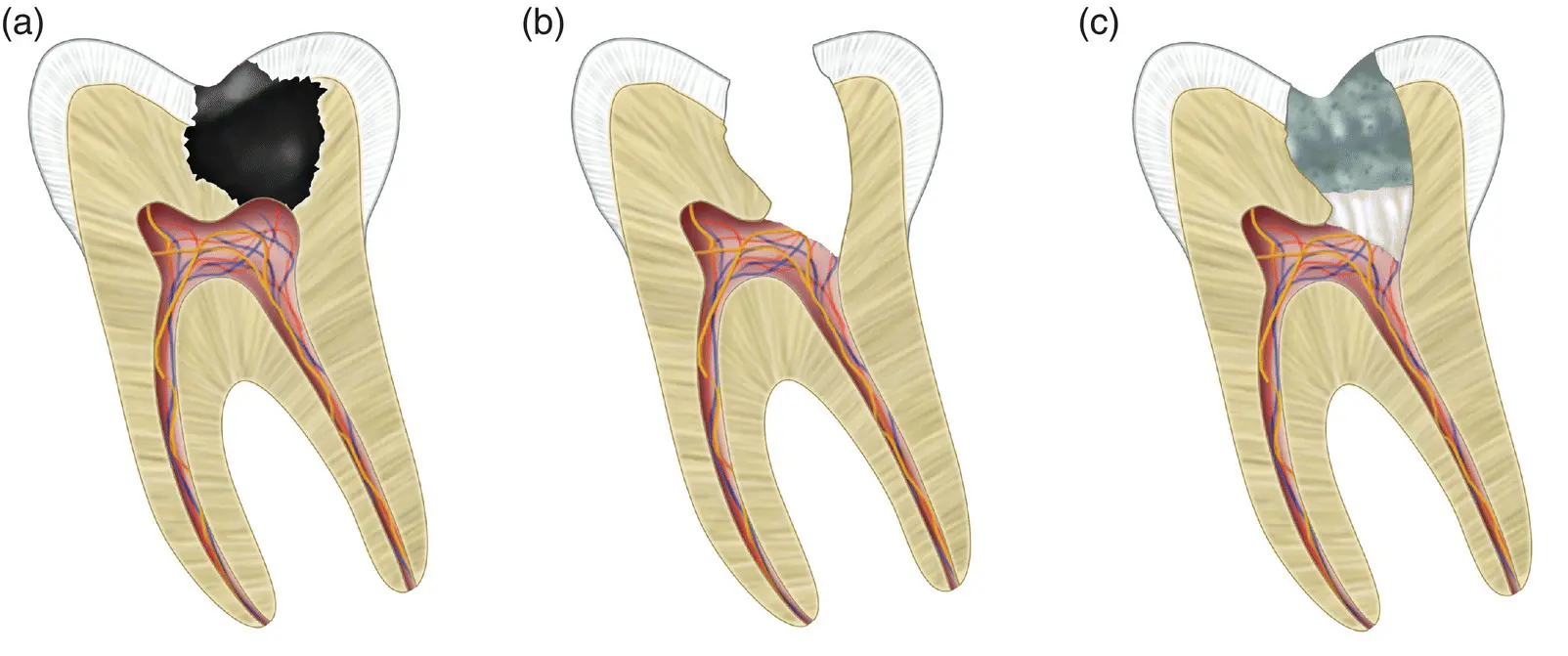
Figure 2.5 Partial pulpotomy. (a) Deep carious lesion extending to the pulp. (b) Removal of the superficial pulp tissue where it is inflamed. (c) Calcium silicate cement directly interfacing with the pulp following definitive restoration.
2.3.3.4 Pulpectomy
For completeness, this procedure is considered here as it is a form of VPT. In treating cases where it is determined that the pulp is not viable as it appears to be severely inflamed or contaminated and haemostasis is unachievable or the pulp appears necrotic, a pulpectomy may be indicated. It has been shown that success rates are higher when the pulpectomy and RCT are completed in one visit, and the clinician should adopt a cautious approach with length control. Pulpectomy is defined as total removal of the pulp from the root canal system followed by RCT ( Figure 2.7).
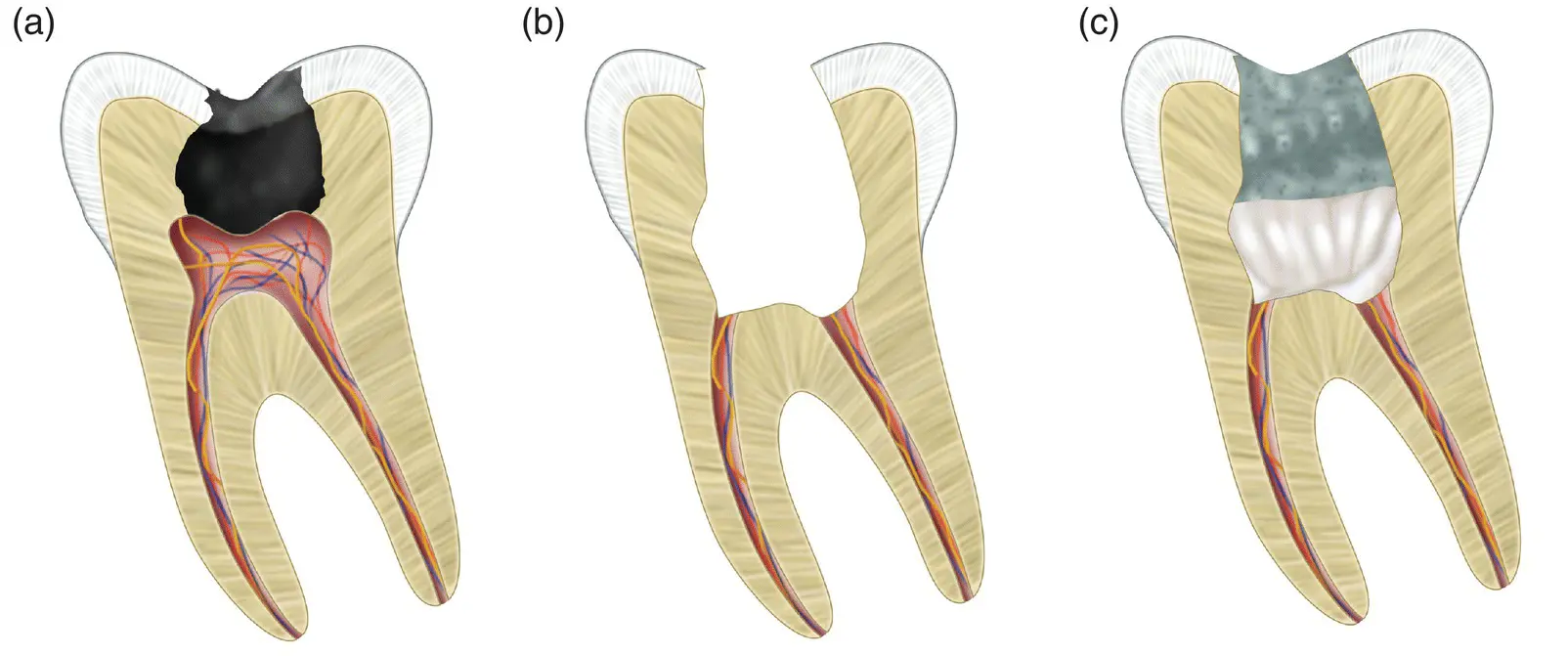
Figure 2.6 Full pulpotomy. (a) Deep carious lesion extending to the pulp. (b) Removal of the whole of the coronal portion of the pulp. (c) Calcium silicate cement directly interfacing with pulp stumps at the canal orifice following definitive restoration.
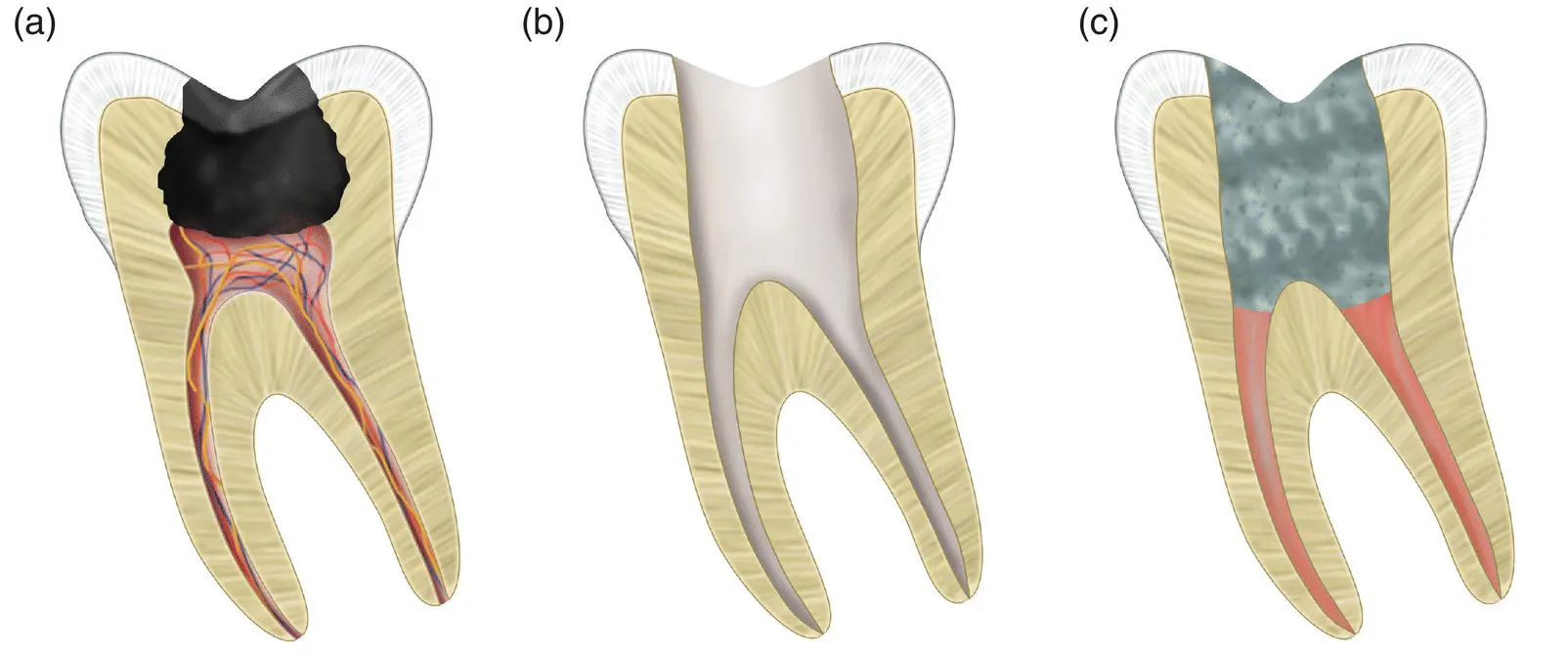
Figure 2.7 Pulpectomy. (a) Deep carious lesion extending to the pulp, resulting in irreversible change. (b) Complete removal of the pulp tissue and cleaning and preparation of the root canal system prior to root filling. (c) Obduration of the root canals with gutta‐percha following definitive restoration.
2.3.4 Immature Roots
VPT is of particular importance in immature permanent teeth where root formation is not complete and the root structure is weak. Successful maintenance of pulp vitality will allow root formation to continue in a process known as apexogenesis. In reality, the term ‘apexogenesis’ is seldom used in modern endodontics, first because it is often confused with apexification, and second because it simply refers to pulp capping: a partial or full pulpotomy procedure carried out in a tooth with an immature root structure. VPT on immature teeth is most commonly carried out following trauma on the anterior teeth, which for practical reasons may be better treated with a partial or ‘Cvek’ pulpotomy, where part of the exposed pulp tissue is removed and a capping material is placed [60]. Young patients presenting with an open apex will have a greater blood supply and increased cellularity of their pulps, which has been suggested to result in more predictable healing [86]. However, the influence of age has not generally been linked to improved healing in VPT [64, 87].
2.4 Materials Used in Vital Pulp Treatment
2.4.1 The Role of the Material
For predictable and successful VPT, careful material selection is required. The demands on the material itself are numerous, as it is situated in a unique environment in which it must interface with vital tissue that has a blood supply, hard dental tissues, and other restorative materials. Historically, numerous different materials have been used in VPT, including gold foil [88], aqueous calcium hydroxide [89], commercial preparations of calcium hydroxide [90], glycyrrhetinic acid/antibiotic mixture [91], resin bonding agents [92], corticosteroid/antibiotic mixture [93], isobutyl cyanoacrylate [94], resin‐modified glass ionomer [95], and, more recently, HCSC [96].
The fundamental aim of any material used in VPT is to maintain a viable pulp so that it can continue normal homeostatic and protective functions of the tooth. As the pulp has the ability to lay down dental hard tissue in the form of reactionary or reparative dentine, the chosen material should promote this response in order to increase the thickness of dentine between the pulp and the deepest part of any cavity ( Figure 2.2). The production of a thicker layer of mineralized tissue over the pulp renders it well protected from future noxious stimuli. Any pulp‐capping material should also have antimicrobial properties, as it is well established that pulp necrosis will not result without the presence of microorganisms [12].
Читать дальшеИнтервал:
Закладка:
Похожие книги на «Endodontic Materials in Clinical Practice»
Представляем Вашему вниманию похожие книги на «Endodontic Materials in Clinical Practice» списком для выбора. Мы отобрали схожую по названию и смыслу литературу в надежде предоставить читателям больше вариантов отыскать новые, интересные, ещё непрочитанные произведения.





Обсуждение, отзывы о книге «Endodontic Materials in Clinical Practice» и просто собственные мнения читателей. Оставьте ваши комментарии, напишите, что Вы думаете о произведении, его смысле или главных героях. Укажите что конкретно понравилось, а что нет, и почему Вы так считаете.