Emergency Management of the Hi-Tech Patient in Acute and Critical Care
Здесь есть возможность читать онлайн «Emergency Management of the Hi-Tech Patient in Acute and Critical Care» — ознакомительный отрывок электронной книги совершенно бесплатно, а после прочтения отрывка купить полную версию. В некоторых случаях можно слушать аудио, скачать через торрент в формате fb2 и присутствует краткое содержание. Жанр: unrecognised, на английском языке. Описание произведения, (предисловие) а так же отзывы посетителей доступны на портале библиотеки ЛибКат.
- Название:Emergency Management of the Hi-Tech Patient in Acute and Critical Care
- Автор:
- Жанр:
- Год:неизвестен
- ISBN:нет данных
- Рейтинг книги:3 / 5. Голосов: 1
-
Избранное:Добавить в избранное
- Отзывы:
-
Ваша оценка:
Emergency Management of the Hi-Tech Patient in Acute and Critical Care: краткое содержание, описание и аннотация
Предлагаем к чтению аннотацию, описание, краткое содержание или предисловие (зависит от того, что написал сам автор книги «Emergency Management of the Hi-Tech Patient in Acute and Critical Care»). Если вы не нашли необходимую информацию о книге — напишите в комментариях, мы постараемся отыскать её.
Provides algorithms for the most common clinical scenarios of device malfunction and related complications Covers management of patients who have undergone major operations such as organ transplantation or complex congenital heart disease repair Presents detailed management plans for a wide range of hardware types and medical conditions Offers expert guidance to practitioners in settings where not all specialties are readily available, such as rural and remote areas or community hospitals Features contributions from a team of experts in various areas of adult and pediatric emergency and critical care medicine
is a must-have clinical reference and guide for pediatric and adult emergency medicine physicians, general pediatricians, internists, general practitioners, critical care specialists, and allied health practitioners.
Emergency Management of the Hi-Tech Patient in Acute and Critical Care — читать онлайн ознакомительный отрывок
Ниже представлен текст книги, разбитый по страницам. Система сохранения места последней прочитанной страницы, позволяет с удобством читать онлайн бесплатно книгу «Emergency Management of the Hi-Tech Patient in Acute and Critical Care», без необходимости каждый раз заново искать на чём Вы остановились. Поставьте закладку, и сможете в любой момент перейти на страницу, на которой закончили чтение.
Интервал:
Закладка:
Gastric Decompression Devices
Similar to the temporary feeding devices, there are NG and OG tubes used for decompression and lavage. These devices are larger than feeding tubes: 8–10 Fr for children and 12–14 Fr for adults. Decompression devices are divided into single and double lumen tubes. Single lumen tubes, such as the Levin tube, are used more frequently in the emergency department or intensive care unit for intermittent decompression. Single lumen tubes should not be placed on continuous suction because they can adhere to the stomach wall and cause tissue damage. A double lumen tube is the preferred decompression device because it has both a large lumen for suction or irrigation and a small lumen (typically blue in color) that vents the large lumen. This small lumen serves as a pop‐off valve for the device to prevent excessive suctioning. There are two common types of double lumen tubes: Salem sumps and Replogle tubes. Salem sumps are preferred in an emergency setting because they have several suction holes along the side of the tubing for rapid efficient suctioning, whereas Replogle tubes have suction holes only at the most distal end of the tube.
When using a double lumen tube, it is critical that the small lumen be kept to room air to adequately vent the large lumen. It should not be clamped, used for suction, or used for irrigation. Finally, the proximal end of a double lumen decompression device must be kept above waist‐height, otherwise the gastric contents may reflux into the small lumen.
Long‐term Feeding Devices
G‐tubes are used for long‐term or permanent enteric feeding. G‐tubes are divided into standard adjustable length tubes and low‐profile (i.e. button) tubes. When caring for a patient with a long‐term feeding device, it is imperative that you know the type of tube the patient has, how the tube was placed, and how to use the tube in order to adequately care for your patient.
Basic G‐tube Anatomy
G‐tubes are made of silicone, polyurethane, or, rarely, latex rubber to provide the flexibility and durability needed for long‐term feeding. They serve as a direct pathway to the gut. G‐tubes are made up of one to three ports on the most proximal end, followed by a tube or shaft that carries nutrition to the gastrointestinal (GI) tract, and then a balloon or nonballoon retention device on the distal end ( Figure 1.1). In some tubes, there are separate feeding and medication ports. Only in balloon G‐tubes is there a port that is used to expand the retention balloon. In addition, standard G‐tubes have an external retention device with air vents and feet that hold it 1–2 mm above the skin surface to prevent skin breakdown and keep the stoma site clean and dry.
There are advantages and disadvantages to balloon and nonballoon G‐tubes. The benefit of balloon G‐tubes is that they can be replaced at home; however, they are not as well tolerated as nonballoon retention devices because of the size of the balloon. Furthermore, balloon retention devices need to be changed more frequently than nonballoon G‐tubes (every three months compared to every six months, respectively). The main disadvantage of nonballoon G‐tubes is that every tube change has to be done by a medical professional.
Standard G‐Tube
Standard G‐tubes are adjustable length tubes that have an external bolster, which sits on the skin and can be moved up and down to adequately secure the tube in a patient of any size ( Figure 1.1a and b). These are particularly helpful in patients with increased soft tissue or in patients with a projected weight gain where a low‐profile tube with a fixed shaft length may not fit properly. Standard G‐tubes can be placed surgically or endoscopically.
Standard G‐tubes are placed surgically using the Stamm procedure or via a laparoscopic approach. You will know your patient had the Stamm procedure if he or she has a 6–8 cm midline incision on examination. During the procedure, the surgeon dissects down to the anterior wall of the stomach. The G‐tube is placed directly into the stomach via an anterior incision. The balloon is inflated and used to pull the stomach against the inner abdominal wall to determine the best location for the percutaneous exit of the tubing. Once this incision is made, the tubing is pulled through the abdominal wall and the tube is anchored in place with sutures. A standard G‐tube placed surgically will have a well‐healed tract within four weeks.
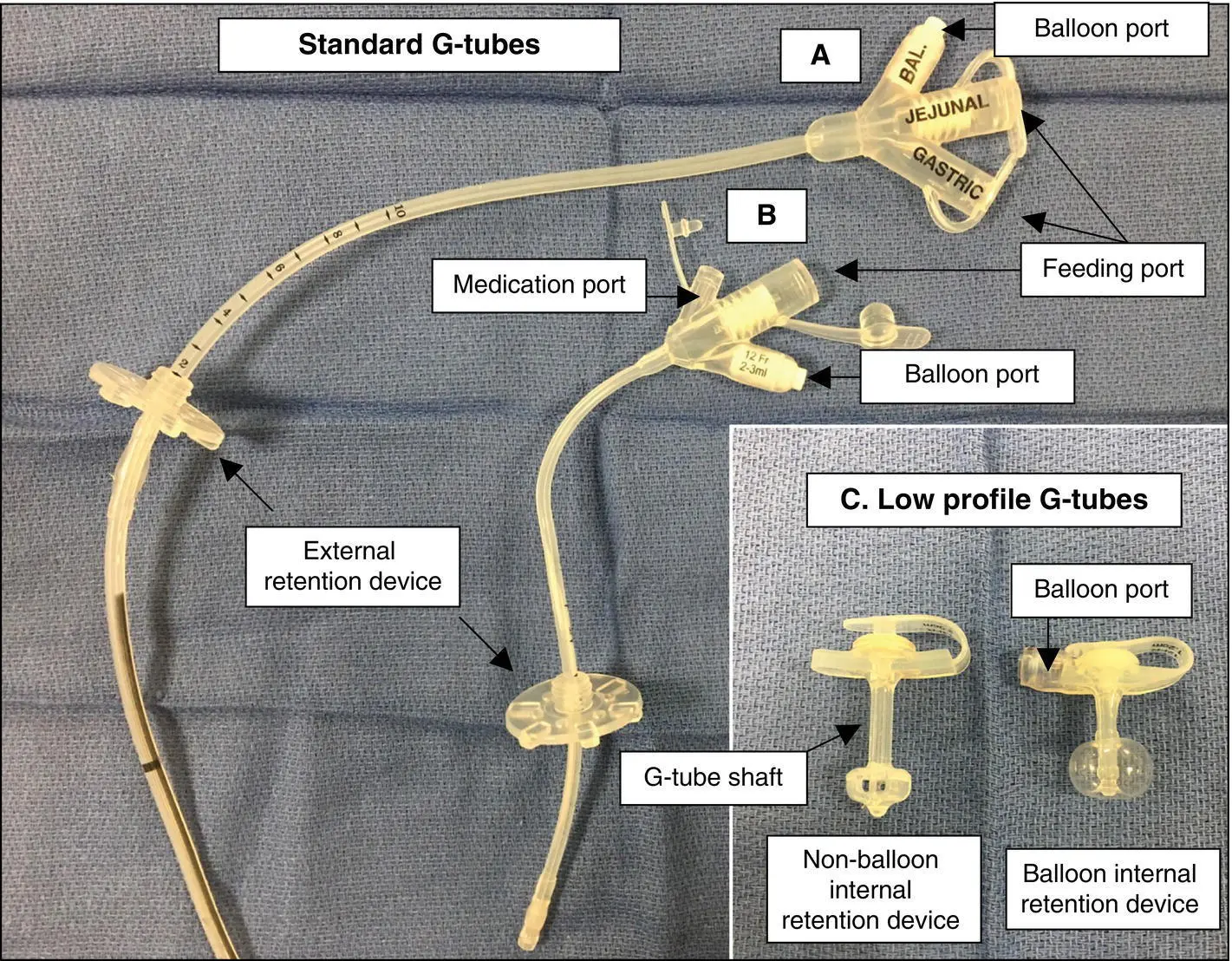
Figure 1.1 Standard G‐tubes and low‐profile G‐tubes. (a) Standard GJ tube with three ports: balloon port, jejunal port, and gastric port. (b) Standard G‐tube with three ports: medication port, gastric port, and balloon port. (c) Low‐profile tubes with both nonballoon and balloon retention devices.
Standard G‐tubes are placed endoscopically by using the percutaneous endoscopic gastrostomy(PEG) technique. Of note, the term “PEG” is used inaccurately in medical vernacular to refer to all kinds of G‐tubes, but a PEG is actually the procedure and not a type of tube. During a PEG procedure, an endoscope is used to transilluminate the stomach and identify the stoma site. A needle is then inserted through the skin into the stomach with a guidewire that is pulled up through the esophagus and out of the mouth. This guidewire is then used to guide the G‐tube into the stomach. A small incision is made, and the G‐tube is pulled through the stomach and abdominal walls and secured in place by the internal and external bolsters alone.
There are two main advantages to a surgically placed G‐tube compared to a PEG procedure. First, a mature tract forms in 4 weeks with a laparoscopic procedure compared to 6–12 weeks with a PEG procedure. Second, a surgically placed G‐tube provides direct visualization of the anatomy, whereas, with an endoscopically placed G‐tube, there is always the risk of a bowel perforation if a portion of bowel is caught between the abdominal wall and the gastric wall during G‐tube placement.
Low‐Profile G‐Tube
Low‐profile G‐tubes have a port that sits flush with the skin surface ( Figure 1.1c). They are more easily hidden than the standard G‐tubes simply by the nature of their size, and patients tend to prefer them for this reason. In addition, the smooth surface of a G‐tube port site without tubing is less prone to accidental dislodgement compared to standard G‐tubes. However, there are drawbacks to a low‐profile tube. First, external tubing has to be attached in order to deliver a feed, which creates one additional step and an additional piece of equipment that can malfunction. Second, low‐profile tubes cannot be adjusted to accommodate increased abdominal wall thickness and must be replaced with a tube that has a longer shaft length when there are signs of abdominal wall compression.
Although they were not designed to be placed primarily, low‐profile G‐tubes can be placed laparoscopically. In pediatric surgical practice, the laparoscopic primary G‐button gastrostomy is now widely performed. In this approach, one trocar is placed through the umbilicus and another through a small incision in the left upper quadrant. A stitch is placed in the anterior wall of the stomach and passed through the trocar in the left upper quadrant. Once the suture material is outside the abdomen, the trocar is removed and the anterior wall is pulled through the initial trocar site. The stomach and abdominal walls are sutured together. The gastrostomy is made in the portion of stomach wall that is exposed. The appropriate button is then placed in the gastrostomy and sutured in place. Similar to a surgically placed standard G‐tube, a low‐profile G‐tube tract matures in four weeks.
Читать дальшеИнтервал:
Закладка:
Похожие книги на «Emergency Management of the Hi-Tech Patient in Acute and Critical Care»
Представляем Вашему вниманию похожие книги на «Emergency Management of the Hi-Tech Patient in Acute and Critical Care» списком для выбора. Мы отобрали схожую по названию и смыслу литературу в надежде предоставить читателям больше вариантов отыскать новые, интересные, ещё непрочитанные произведения.







Обсуждение, отзывы о книге «Emergency Management of the Hi-Tech Patient in Acute and Critical Care» и просто собственные мнения читателей. Оставьте ваши комментарии, напишите, что Вы думаете о произведении, его смысле или главных героях. Укажите что конкретно понравилось, а что нет, и почему Вы так считаете.