Manual of Equine Anesthesia and Analgesia
Здесь есть возможность читать онлайн «Manual of Equine Anesthesia and Analgesia» — ознакомительный отрывок электронной книги совершенно бесплатно, а после прочтения отрывка купить полную версию. В некоторых случаях можно слушать аудио, скачать через торрент в формате fb2 и присутствует краткое содержание. Жанр: unrecognised, на английском языке. Описание произведения, (предисловие) а так же отзывы посетителей доступны на портале библиотеки ЛибКат.
- Название:Manual of Equine Anesthesia and Analgesia
- Автор:
- Жанр:
- Год:неизвестен
- ISBN:нет данных
- Рейтинг книги:3 / 5. Голосов: 1
-
Избранное:Добавить в избранное
- Отзывы:
-
Ваша оценка:
Manual of Equine Anesthesia and Analgesia: краткое содержание, описание и аннотация
Предлагаем к чтению аннотацию, описание, краткое содержание или предисловие (зависит от того, что написал сам автор книги «Manual of Equine Anesthesia and Analgesia»). Если вы не нашли необходимую информацию о книге — напишите в комментариях, мы постараемся отыскать её.
Provides practical, clinically oriented information on anesthetizing equids Uses a bulleted format designed for fast access of key information Offers step-by-step instructions and diagrams of nerve blocks of the limbs, head, and ophthalmic structures Includes new coverage of topics including regulation of extracellular fluid and blood pressure, acid-base disorders, and hemodynamic effects of autonomic drugs
remains a must-have resource for all equine practitioners and veterinary students involved with anesthetizing horses.
Manual of Equine Anesthesia and Analgesia — читать онлайн ознакомительный отрывок
Ниже представлен текст книги, разбитый по страницам. Система сохранения места последней прочитанной страницы, позволяет с удобством читать онлайн бесплатно книгу «Manual of Equine Anesthesia and Analgesia», без необходимости каждый раз заново искать на чём Вы остановились. Поставьте закладку, и сможете в любой момент перейти на страницу, на которой закончили чтение.
Интервал:
Закладка:
Inhibitory neurotransmitters include glycine, gamma aminobutyric acid (GABA), enkephalins, and endorphins.
Other transmitters include neurotensin, thyroid‐releasing hormone (TRH), gonadotropin‐releasing hormone (GnRH), melanocyte stimulating releasing‐inhibitory factor, adrenocorticotropic hormone (ACTH), and somatostatin.
C Brain metabolism
The brain almost exclusively uses glucose as a source of energy. The brain can also use two ketones, 3‐hydroxybutyrate and acetoacetate.
The selectivity of the blood–brain barrier makes the brain dependent on glucose as an energy substrate, and low concentrations decrease the level of consciousness.
Twenty‐five percent of glucose is used for energy, and the remainder is used for protein synthesis (e.g. glutamic and aspartic acid) which are also used for energy in some cell pathways.
D Cerebral blood flow
Cerebral blood flow increases with cerebral oxygen demand (especially when PaO2 decreases below 50 mmHg) and increases linearly with PaCO2 over the range 20–80 mmHg (see Figure 6.1).
Hypothermia blunts the response to changing PaCO2.
The response to CO2 is maintained during volatile and intravenous anesthesia.
Normal cerebral blood flow in humans is 50 ml/100 g/minute and it has not been quantified in horses.
Flow is greatest in neonates and declines with age, and within gray matter (80 ml/100 g/minute).
Autoregulation maintains constant brain–blood flow over a range of mean systemic blood pressures (60–130 mmHg). Autoregulation is dependent on two processes:Vascular smooth muscle responses which occur over 30–40 seconds.Neural mediated vasodilation through cranial nerve VII.
Arterial hypercapnia or hypoxemia, atropine, and volatile anesthesia administration may attenuate or abolish autoregulation.
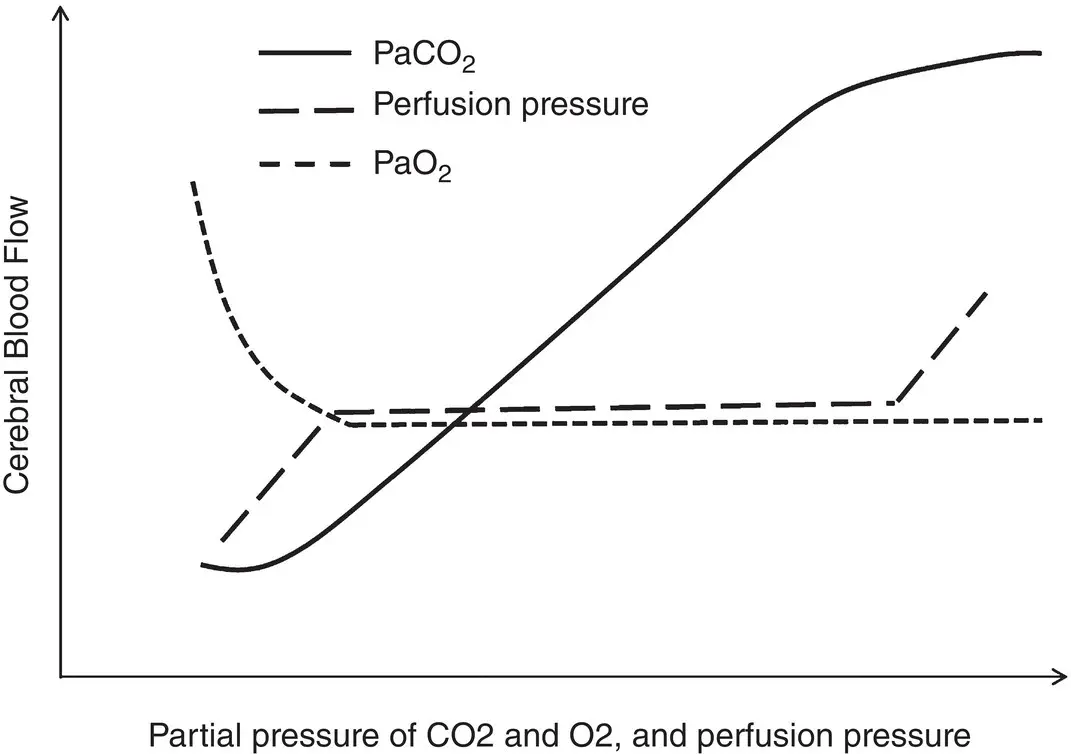
Figure 6.1 The effects of arterial partial pressure of O 2and CO 2, and perfusion pressure on cerebral blood flow.
E Cerebral perfusion pressure ( CPP)
Intracranial pressure (ICP) is maintained at approximately 2 mmHg in conscious healthy horses, even when the head is lowered below heart level.
Normal neonatal foals in the first 24 hours after birth have ICP between 2 and 15 mmHg and a CPP of in the range 50–109 mmHg.
Mean (SD) values for ICP in adult standing horses are 2 (4) mmHg and for CPP are 102 (26) mm Hg.
Cerebral perfusion pressure is the difference between systemic mean arterial blood pressure and ICP, and should be at least 60 mmHg.
When CPP is below this value or cardiac output decreases to less than half‐normal values, cerebral circulation becomes insufficient.
In isoflurane‐anesthetized horses maintained at 1.2 MAC, ICP increases and is higher in dorsal than in lateral and sternal recumbency (34 vs 24 vs 19 mmHg, respectively). Head down position for dorsal and sternal recumbency increases ICP further. Because MAP is higher (105 mmHg) in sternal recumbency, CPP is higher (71 mmHg for sternal with head up and 87 mmHg for sternal with head down); intermediate for dorsal recumbency (MAP of 85 mmHg for head level with the thorax and CPP of 51 mmHg; MAP of 76 mmHg for head down and CPP of 55 mmHg); and lower for lateral recumbency (MAP of 72 mmHg and CPP of 48 mmHg).
Increasing end‐tidal concentrations of the inhalational anesthetic causes significant dose‐dependent decreases in MAP and CPP, but no change in ICP.
Mechanical ventilation causes a significant decrease in MAP and ICP but no change in CPP.
F Cerebrospinal fluid ( CSF)
CSF is continuously formed by the choroid plexuses in the lateral and third ventricles and has a specific gravity of 1.002–1.009. The fluid passes into the fourth ventricle, and then into the subarachnoid space around the brain and spinal cord through three foramina.
Most absorption occurs through the subarachnoid villi which protrude into the venous sinuses of the cranium.
The subarachnoid space does not communicate with the subdural space, but is continuous with the ventricles of the brain through medial and lateral connections in the roof of the fourth ventricle. Separations of the arachnoid and pia mater form the cerebro‐medullary cistern or cisterna magna.Samples of CSF can be obtained from lumbar puncture or through the cisterna magna, although the latter technique carries a higher risk.
CSF is exchanged every four hours and absorption helps maintain pressure at a constant level.
CSF acts as a cushion and support for the brain.
Changes in brain volume can be offset by CSF production and absorption.
The composition of CSF is tightly regulated. CSF pH remains about 7.33 even with wide changes in plasma pH. Compared to other extra‐cellular fluids, CSF contains 7% higher sodium and chloride ion, and 30% and 40% lower glucose and potassium concentrations, respectively.
A CSF pH decrease of 0.05 units rapidly results in a fourfold increase in ventilation and reflects the ability of lipid soluble CO2 to cross the blood–brain‐barrier, not hydrogen ions. Active transport of bicarbonate ions returns CSF pH to normal with chronic changes in arterial pH.
A potential difference between CSF and blood of about +5 mV is the result of an active transport system.
O2, CO2, barbiturates, glucose, and lipophilic (anesthetic and sedative) substances effectively cross the blood–brain barrier.
Inorganic ions, highly dissociated compounds, amino acids, and sucrose cross very slowly.
CSF pressure changes with body position, and expiratory efforts such as coughing or straining can sharply increase the pressure.
II Central nervous system pathophysiology
A Seizures
Seizures are not common in horses and classification and diagnosis is reviewed elsewhere.
Accidental injection of drugs into the carotid artery can cause convulsions.
Anticonvulsants raise the seizure threshold, prevent spread of seizure activity, and decrease the level of activity of abnormal neurons while sparing normal cells.
B Intracranial pressure (ICP) increase
As an intracranial mass expands within the bony cranium it can cause an increase in ICP. This increase in ICP can be offset by displacement of CSF, blood flow, and displacement of the brain matter.This effect does not continue, and once a certain point is reached, ICP can rise exponentially (see Figure 6.2).
Sudden increases in ICP can increase the risk of brain herniation.
During neuroanesthesia, steps are taken to reduce brain volume as much as possible to offset increases in ICP.
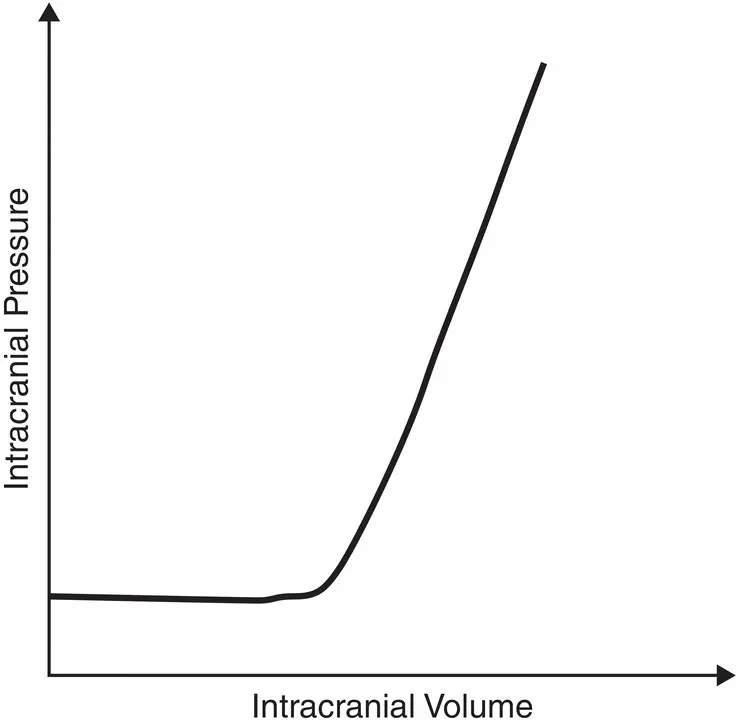
Figure 6.2 The effects of intracranial volume changes on intracranial pressure. At a certain point, the increase in intracranial volume causes a dramatic increase in intracranial pressure as compensatory mechanisms become exhausted.
III Neuroanesthesia
Anesthetic drugs and manipulations performed during anesthesia can affect:
A Cerebral metabolic rate
In humans, normal O2 consumption is 3–5 ml/100 g/minute, similar to that of working skeletal muscle.
When the level of consciousness is depressed, the cerebral metabolic rate is decreased.
Читать дальшеИнтервал:
Закладка:
Похожие книги на «Manual of Equine Anesthesia and Analgesia»
Представляем Вашему вниманию похожие книги на «Manual of Equine Anesthesia and Analgesia» списком для выбора. Мы отобрали схожую по названию и смыслу литературу в надежде предоставить читателям больше вариантов отыскать новые, интересные, ещё непрочитанные произведения.




Обсуждение, отзывы о книге «Manual of Equine Anesthesia and Analgesia» и просто собственные мнения читателей. Оставьте ваши комментарии, напишите, что Вы думаете о произведении, его смысле или главных героях. Укажите что конкретно понравилось, а что нет, и почему Вы так считаете.