A Practical Approach to Special Care in Dentistry
Здесь есть возможность читать онлайн «A Practical Approach to Special Care in Dentistry» — ознакомительный отрывок электронной книги совершенно бесплатно, а после прочтения отрывка купить полную версию. В некоторых случаях можно слушать аудио, скачать через торрент в формате fb2 и присутствует краткое содержание. Жанр: unrecognised, на английском языке. Описание произведения, (предисловие) а так же отзывы посетителей доступны на портале библиотеки ЛибКат.
- Название:A Practical Approach to Special Care in Dentistry
- Автор:
- Жанр:
- Год:неизвестен
- ISBN:нет данных
- Рейтинг книги:3 / 5. Голосов: 1
-
Избранное:Добавить в избранное
- Отзывы:
-
Ваша оценка:
A Practical Approach to Special Care in Dentistry: краткое содержание, описание и аннотация
Предлагаем к чтению аннотацию, описание, краткое содержание или предисловие (зависит от того, что написал сам автор книги «A Practical Approach to Special Care in Dentistry»). Если вы не нашли необходимую информацию о книге — напишите в комментариях, мы постараемся отыскать её.
Learn to treat dental patients with disabilities or who are medically compromised A Practical Approach to Special Care in Dentistry
A Practical Approach to Special Care in Dentistry
A Practical Approach to Special Care in Dentistry — читать онлайн ознакомительный отрывок
Ниже представлен текст книги, разбитый по страницам. Система сохранения места последней прочитанной страницы, позволяет с удобством читать онлайн бесплатно книгу «A Practical Approach to Special Care in Dentistry», без необходимости каждый раз заново искать на чём Вы остановились. Поставьте закладку, и сможете в любой момент перейти на страницу, на которой закончили чтение.
Интервал:
Закладка:
3 You decide it would be better to control the acute infection in #54 and extract the tooth at a later date. What should you consider when prescribing antibiotics?Administration of antibiotics can alter the blood glucose level and require an insulin dose adjustmentCoeliac disease may affect the absorption of antibiotics; antibiotics known to be associated with an increased risk of gastrointestinal toxicity should be avoidedAvoid azithromycin and metronidazole because they boost the action of hypoglycaemic agents
4 What factors are considered important in assessing the risk of managing this patient?SocialConsent: the parents are divorced and do not have a good relationship; their opinion regarding the proposed extraction of the #54 may differ (although there can be legal differences in the law from one country to another)Anxiety may be heightened due to the above social factorsLimited co‐operationMedicalHypoglycaemia risk: unable to eat properly due to the dental pain; fasting after dental procedures can also trigger a hypoglycaemic episodeHyperglycaemia risk: emotional and surgical stress can result in increased glucose levelsReduced co‐operation may be misinterpreted as related to generalised anxiety instead of abnormal glucose levelsEfficacy of oral medication may be impacted by poor absorption secondary to coeliac diseaseDentalIncreased susceptibility to infectionLikelihood of delayed healing after dental extractionIncreased caries risk (xerostomia; father does not assist with toothbrushing)Coeliac disease can cause enamel defects and mouth ulcers (as observed for this patient)Delayed dental development (coeliac disease and diabetes)
5 The patient injects a daily dose of fast‐acting insulin at 8 a.m. and a dose of long‐acting insulin at 10 p.m. At what time should you schedule the dental extraction?Fast‐acting insulin will have its peak effect between 9 a.m. and noonLong‐acting insulin will have its peak effect around 10 a.m.Ideally, the treatment should be performed in the morning, because the risk of hypoglycaemia is lower when the concentration of endogenous corticosteroids increases. This should be as soon as possible after breakfast (also avoids interfering with the next meal)
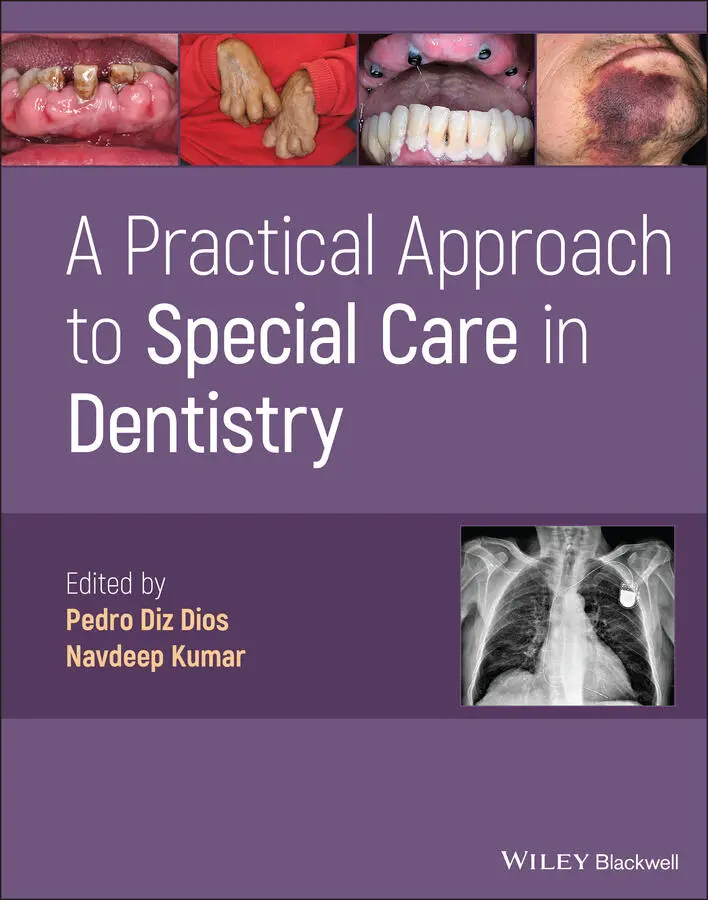
6 What laboratory tests are recommended before the tooth extraction?Serum glucose concentration before starting the procedureRecent HbA1c reading to determine the degree of metabolic control; postpone treatment if HbA1c >9% Figure 5.1.2 (a–c) Severe periodontal disease in a 37‐year‐old male with diabetes mellitus.
General Dental Considerations
Oral Findings
Occasionally, oral findings can represent an initial manifestation of undiagnosed diabetes
Periodontal disease is the most common oral finding ( Figure 5.1.2). Its pathogenesis involves vascular changes (microangiopathy), neutrophil dysfunction and collagen metabolism deficiencies. The presence of periodontitis impedes glycaemic control and contributes to the onset of other extraoral complications
Susceptibility to bacterial (including odontogenic abscesses) and fungal infections (such as oral candidiasis and mucormycosis in the sinuses)
Xerostomia, which can favour the onset of caries ( Figure 5.1.3). Chronic bilateral and asymptomatic inflammation of the parotid glands (sialosis) can develop as a compensatory mechanism
Burning mouth syndrome (probably related to peripheral neuropathy)
Circumoral paraesthesia (associated with peripheral neuropathy)
Glossitis, loss of the filiform papillae and dysgeusia Figure 5.1.3 Xerostomia – depapillated, smooth dry dorsum of the tongue.
High prevalence of oral lichen planus
Mucosal lichenoid reactions and facial flushing (secondary effects of antidiabetic drugs)
Delayed tooth eruption
Dental Management
The dental treatment plan will be determined mainly by the patient's previous oral health and degree of metabolic control ( Table 5.1.1)
The dental team should be aware of how to manage hypoglycaemic events in the dental clinic ( Table 5.1.2)
Section II: Background Information and Guidelines
Definition
Diabetes mellitus is a chronic metabolic disorder characterised by a relative or absolute absence of insulin. Although various types of diabetes have been described (type 1, type 2 and gestational), all are characterised by high blood glucose levels. Worldwide, there are more than 420 million individuals with diabetes (approximately 9% of the worldwide adult population), although it has been estimated that more than 40% of cases are still undiagnosed.
Aetiopathogenesis
Type 1 diabetes: ~8% (previously known as insulin‐dependent or juvenile‐onset)The beta cells in the pancreas produce little or no insulinExogenous insulin must therefore be administered throughout the patient's lifeMost cases have an autoimmune aetiology, although some are idiopathic
Type 2 diabetes: ~90% (previously known as non‐insulin‐dependent or adult‐onset)The insulin receptors in the target tissues show reduced sensitivity to the action of insulin (insulin resistance), although insulin production can be normalAs the disease progresses, a lack of insulin may also developGenerally associated with a genetic predisposition, obesity or metabolic syndrome (combination of diabetes, hypertension and obesity)
Gestational diabetesTriggered by an increase in insulin resistance that causes impaired glucose tolerance during pregnancy
Secondary diabetes can be caused by endocrinopathies (e.g. acromegaly, Cushing disease), drugs (e.g. corticosteroids) or pancreatic disease (surgery, tumour or inflammation)
Clinical Presentation
Type 1: usually presents before the age of 40 years
Type 2: average age of onset is 45 years old
Classic symptoms, especially those of undiagnosed type 1 diabetesPolyuria (frequent voiding), polydipsia (excessive thirst) and polyphagia (excessive hunger)Fatigue, infections, slow wound healing, blurred vision, weight loss
Hypoglycaemia (onset can be rapid; more frequent; life‐threatening)Early signs/symptoms: shakiness, dizziness, sweating, hunger, piloerection, tachycardia, inability to concentrate, confusion, irritability or moodiness, anxiety (due to increased epinephrine activity) or nervousness, headacheLater signs/symptoms: clumsiness or jerky movements, inability to eat or drink, muscle weakness, difficulty speaking or slurred speech, blurry or double vision, drowsiness, confusion, convulsions or seizures, unconsciousness, death
Hyperglycaemia (slower onset, more protracted course)Early signs/symptoms: frequent urination, increased thirst, blurred vision, fatigue, headacheLater signs/symptoms: fruity‐smelling breath, nausea and vomiting, shortness of breath, dry mouth, weakness, confusion, abdominal pain, coma Table 5.1.1 Considerations for dental management.Risk assessmentHypoglycaemia is the main risk and must be managed urgently (see Ta ble 5.1.2)HyperglycaemiaFatigue/reduced tolerance for long treatmentIncreased risk of infectionPoor wound healingIncreased risk of periodontal diseaseComplications related to comorbidities/secondary vascular complicationsCriteria for referralIf HbA1c levels are <7%, any type of dental treatment can generally be performed within the dental clinicFor patients with poorly controlled diabetes (HbA1c >9%), only emergency treatments should be conducted and surgical procedures should preferably be undertaken in a hospital settingWith HbA1c readings >12%, all procedures should be postponed until the glycaemic control has improvedAccess/positionThe sessions should preferably be scheduled for the morning (higher endogenous cortisol levels increase blood glucose and decrease the risk of hypoglycaemia)Avoid scheduling an appointment time that coincides with the maximum insulin activity peak or when it may lead to a meal being missedCommunicationA significant percentage of individuals with diabetes are unaware of their conditionPatients with signs/symptoms or oral findings suggestive of diabetes should be referred to their doctor for investigationCommunication may be impaired if blood glucose levels are not controlled (slurred speech, confusion)Consent/capacityPatients should be informed that the dental treatment plan and its success will be determined by the degree of diabetic control (e.g. success rates for dental implants are lower for patients with suboptimal diabetes control)Patients should be warned of the potential for local and systemic complications resulting from diabetes (increased infection risk, delayed healing)If diabetic control is poor, the patient may be confused, anxious and/or agitated – this will reduce their capacity to give consentAnaesthesia/sedationLocal anaesthesiaAny local anaesthetic may be employed by following the routine precautionsSedationControlling the patient's stress is importantFor patients with poor metabolic control and comorbidities, sedation should be performed in a hospital settingGeneral anaesthesiaThe use of general anaesthesia is determined by the severity of the comorbiditiesDental treatmentBeforeConfirm that the patient has eaten normally and has taken the scheduled medicationThe presence of an oral infection and the administration of antibiotics can change the insulin requirements and might require adjustment by a physicianThe physician should also be consulted if the planned procedure is expected to change the normal eating habitsFor an oral surgical or periodontal procedure, anticipate the postintervention fasting/changes in dietAssess the need for antibiotic prophylaxis (not supported by scientific evidence)Performing a new rapid HbA1c test may be consideredDuringDental implants can be placed successfully in patients with well‐controlled diabetesThe main complication during dental treatment is hypoglycaemiaAfterSlow healing of the surgical wound is commonDue to the increased risk of infection, consider the need for postoperative antibiotics, if an invasive procedure is undertaken (especially for patients with poor disease control)Once the session has finished, slowly sit the patient up from the supine position (postural hypotension due to autonomic neuropathy)Periodontal treatment has been shown to produce a modest improvement in glycaemic controlIt has been suggested that the success rate of endodontic treatment is lower than that for the general population, especially for patients with poorly controlled diabetes (as has been reported for dental implants)Drug prescriptionThe antibiotic of choice is amoxicillinAvoid using metronidazole and azithromycin because they can boost oral hypoglycaemic agentsAvoid ciprofloxacin because it can compete with insulinThe analgesic of choice is paracetamolAvoid using aspirin, ibuprofen, diclofenac and naproxen because they can boost oral hypoglycaemic agentsAvoid corticosteroids because they can decrease the efficacy of oral hypoglycaemic agentsEducation/preventionPatients with diabetes usually recognise the signs and symptoms of hypoglycaemia. In any case, dentists should know how to identify and manage urgent episodes, especially hypoglycaemia (see Ta ble 5.1.2)Maintaining optimal oral hygiene and regular reviews, with a specific focus on periodontal disease, should be routine for patients with diabetesRemoving any removable prosthesis at night and renewing them periodically are essential for preventing denture‐induced stomatitis Table 5.1.2 Managing hypoglycaemia in the dental clinic a .Alert/responsive patientCheck blood glucose levelIf <3.0 mmol/L (54 mg/dL), give glucose/sugary drink or pure glucose (2 tablets)Recheck blood glucose level after 10–15 minutesGive the patient a complex carbohydrate (biscuits, sandwiches, etc.) to ensure that a sustained release of glucose is maintainedConfused patientCheck blood glucose levelIf <3.0 mmol/L (54 mg/dL), give sublingual dextrose gel (repeated at 10–15 minutes)Recheck blood glucose level after 10–15 minutesAs the level increases, give the patient a complex carbohydrate (biscuits, sandwiches, etc.) to ensure that a sustained release of glucose is maintainedUnconscious patient (blood glucose <2.8 mmol/L or 50 mg/dL)Call for medical assistanceIntramuscular glucagon 1 mg (adults/children over the age of 8 years); 0.5 mg for children under the age of 8 years; not as effective if a patient has liver disease or is anorexicMonitor airway, breathing and circulation throughout aUK Resuscitation Council.
Читать дальшеИнтервал:
Закладка:
Похожие книги на «A Practical Approach to Special Care in Dentistry»
Представляем Вашему вниманию похожие книги на «A Practical Approach to Special Care in Dentistry» списком для выбора. Мы отобрали схожую по названию и смыслу литературу в надежде предоставить читателям больше вариантов отыскать новые, интересные, ещё непрочитанные произведения.







Обсуждение, отзывы о книге «A Practical Approach to Special Care in Dentistry» и просто собственные мнения читателей. Оставьте ваши комментарии, напишите, что Вы думаете о произведении, его смысле или главных героях. Укажите что конкретно понравилось, а что нет, и почему Вы так считаете.