Ridley's The Vulva
Здесь есть возможность читать онлайн «Ridley's The Vulva» — ознакомительный отрывок электронной книги совершенно бесплатно, а после прочтения отрывка купить полную версию. В некоторых случаях можно слушать аудио, скачать через торрент в формате fb2 и присутствует краткое содержание. Жанр: unrecognised, на английском языке. Описание произведения, (предисловие) а так же отзывы посетителей доступны на портале библиотеки ЛибКат.
- Название:Ridley's The Vulva
- Автор:
- Жанр:
- Год:неизвестен
- ISBN:нет данных
- Рейтинг книги:3 / 5. Голосов: 1
-
Избранное:Добавить в избранное
- Отзывы:
-
Ваша оценка:
Ridley's The Vulva: краткое содержание, описание и аннотация
Предлагаем к чтению аннотацию, описание, краткое содержание или предисловие (зависит от того, что написал сам автор книги «Ridley's The Vulva»). Если вы не нашли необходимую информацию о книге — напишите в комментариях, мы постараемся отыскать её.
Ridley’s The Vulva
Ridley’s The Vulva
Ridley's The Vulva — читать онлайн ознакомительный отрывок
Ниже представлен текст книги, разбитый по страницам. Система сохранения места последней прочитанной страницы, позволяет с удобством читать онлайн бесплатно книгу «Ridley's The Vulva», без необходимости каждый раз заново искать на чём Вы остановились. Поставьте закладку, и сможете в любой момент перейти на страницу, на которой закончили чтение.
Интервал:
Закладка:
The fallopian tubes, uterus, and cervix develop from the upper un‐fused portions of the paramesonephric ducts and the vagina from the lower fused portion ( Figure 1.11a). The arrival of the caudal end of the genital canal on the urogenital sinus stimulates cellular proliferation of the sinus epithelium to form three projections (sinuvaginal bulbs) which displace the genital canal dorsally ( Figure 1.11b). Failure of these bulbs to develop results in vaginal agenesis. These sinuvaginal bulbs become solid and together with the solid end of the genital canal form the vaginal plate, which is complete at 19 weeks ( Figure 1.11c). The sinuvaginal bulbs later fuse, but eventually undergo apoptosis to form a lumen. Sometime between 14 weeks and 20 weeks, the vagina opens into the pelvic portion of the urogenital sinus, forming the vaginal vestibule ( Figure 1.11d)
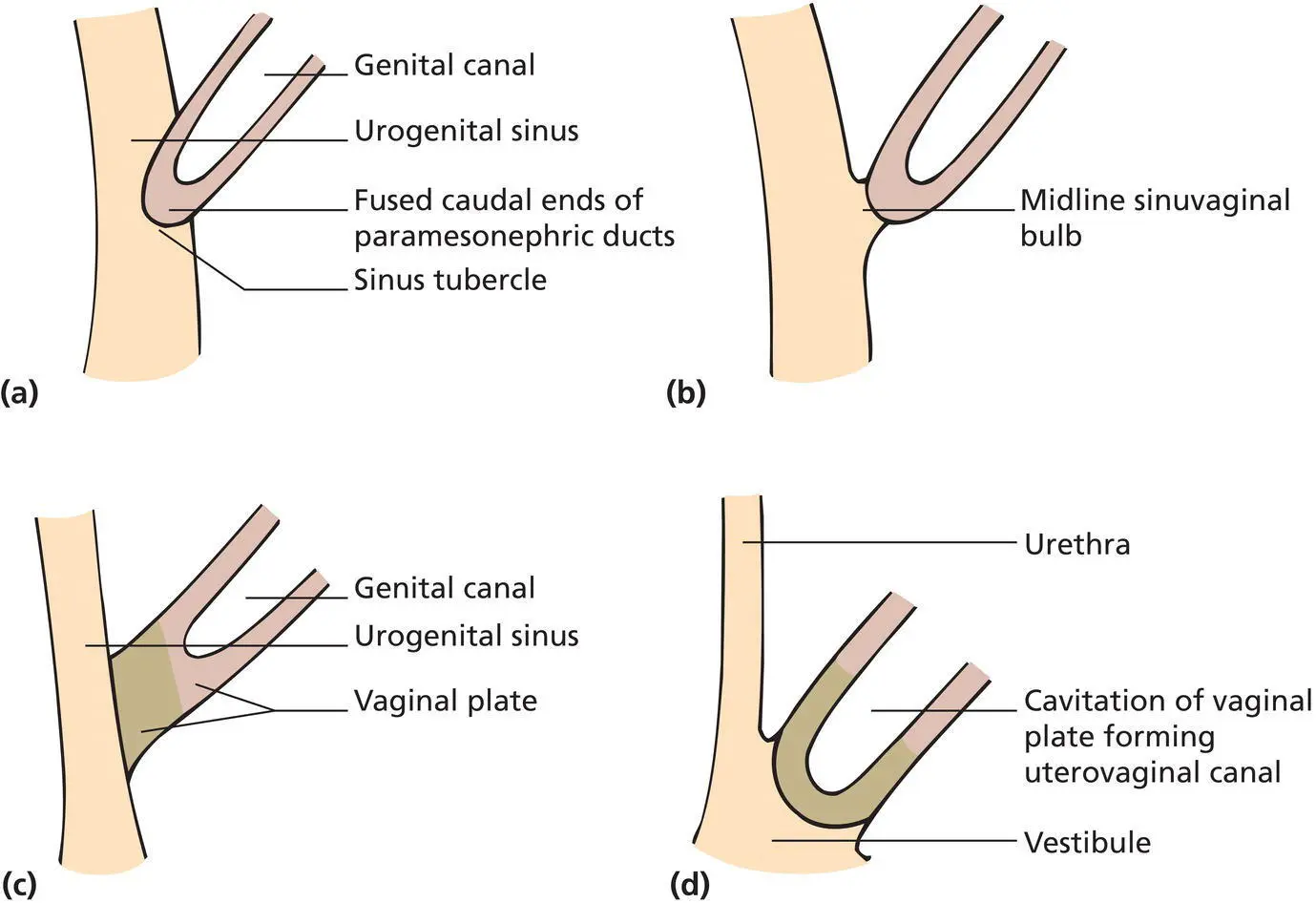
Figure 1.11 (a) The fused paramesonephric ducts form the genital canal, the solid caudal end of which abuts on the posterior wall of the urogenital sinus at the sinus tubercle. (b) Cellular proliferation of the sinus epithelium generates the sinuvaginal bulbs, which displace the genital canal dorsally. (c) Further cellular proliferation converts the sinuvaginal bulbs into solid tissue projections, which participate in the formation of the vaginal plate. (d) Extensive caudal growth of the vaginal plate brings its lower surface into the primitive vestibule.
Further feminisation of the external genitalia begins between 63 and 77 days, when the genital tubercle lengthens to form the phallus. This then bends caudally to form the glans of the clitoris. During this period, the anogenital distance remains unchanged, there is no fusion of the genital folds, and the urogenital sinus remains open. The urethral and vaginal openings separate later. The phallus becomes the clitoris, being incorporated within the fused anterior ends of the genital folds, which develop into the labia minora. The genital swellings lateral to the labia minora become the labia majora and are continuous with the future mons pubis. The labia minora develop from the genital folds and divide anteriorly into the prepuce and frenulum of the clitoris ( Figure 1.12).
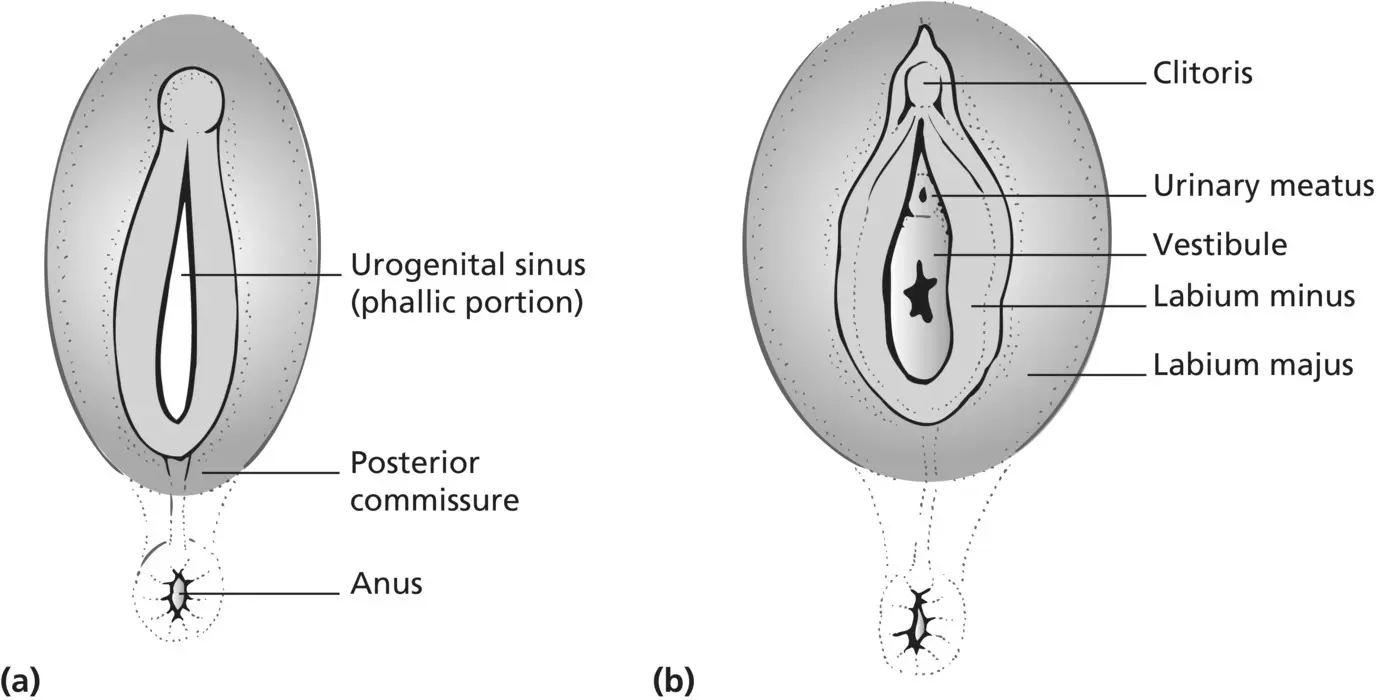
Figure 1.12 (a) The genital and anal membranes rupture. (b) In the female foetus, the urogenital sinus remains open as caudal growth of the vaginal plate brings the urethral and vaginal openings into this region, converting it into the vestibule.
Development of the epithelia
The epidermis of the vulval skin and its appendages – hair, sebaceous and sweat glands – develop from the ectoderm with the dermis developing from the mesoderm. The primitive epidermis is established about the eighth day when the ectoderm differentiates within the developing embryo. At this stage, the epidermis is a single layer of cells, but then a second outer layer develops, the periderm, beneath which the primitive epidermis begins the process of stratification. Keratinisation occurs at the end of the sixth month, and the periderm is sloughed into the amniotic fluid. Cells that are shed from the stratum corneum combine with sebaceous secretions to form the vernix, which makes the embryo impervious to the amniotic fluid and persists until birth.
Three cell types invade the developing epidermis during the first 6 months of intrauterine life. Melanocytes, derived from neural crests, and Langerhans cells, derived from the mesoderm, are present at the end of the third month, while Merkel cells, the origin of which is uncertain, are present by the sixth month [14,15].
The dermo–epidermal junction is flat in all parts of the body until hair and glandular primordia reach the dermis. Primary vellus hair follicles begin to form during the third month of gestation, and the process proceeds in a cephalocaudal manner. Secondary follicles form in close association with the primary follicles, and it is thought that the full complement of hair follicles is present at birth.
Sebaceous glands arise as buds mostly from the hair follicles. They begin to appear during the fourth month and rapidly differentiate into sebum‐producing cells. The development and function of sebaceous glands before birth and in the neonatal period is thought to be regulated by maternal androgens and endogenous foetal steroids. At birth, the glands are large and well developed over the entire body and display the same regional variation in size as is seen in the adult. Postnatally they involute and remain quiescent until puberty.
Eccrine sweat glands start to appear during the third month of prenatal life, and their ducts are open to the skin surface by the sixth month. The premature infant usually shows an absent or limited sweating response [16], even though the glands are innervated as soon as they develop. The number of sweat glands, like hair follicles, seems to be complete at birth.
Apocrine development occurs at sixth months of intrauterine life, and it has been suggested that their primordia develop in association with each hair follicle but then regress in all areas except the areola, axilla, scalp, eyelids, external auditory meatus, umbilicus, and anogenital region [17]. The glandular activity begins during the last trimester, but ceases soon after birth – but then begins again at puberty.
The dermis originates from the mesoderm in the second month of embryonic life. The mesodermal cells form fibroblasts, macrophages, melanoblasts, and mast cells with the matrix composed of collagen and elastin. The organisation of the dermis is progressive throughout gestation and is not complete until some months after birth.
There has been debate about the origin of the vaginal epithelium, but more recent molecular studies, including those of PAX2 and FOXa1 immunostaining [ 18, 19], support a derivation from the urogenital sinus epithelium, as originally suggested [20].
Disorders of sexual development
Normal sexual development is dependent on several activating, repressing, and genetic factors. Disorders of sexual development (DSDs) include a range of conditions that can affect the internal and external genital [ 21]. They may be recognised at birth as the phenotypical appearance may not be characteristic of either male or female. However, the problem can also present at a later stage with an increasing virilised appearance of the genitalia, delayed or absent puberty, or infertility. These patients must be managed in specialist centres by a multidisciplinary team for discussion of management and the timing of any surgical intervention [ 22]. There are ethical issues and patient opinion to be taken into account, and there are guidelines for referral to specialist paediatric endocrinology services for advice and management [ 23].
The classification of DSDs has been revised [ 24], and Table 1.2shows the currently accepted method of categorising these conditions. Terms such as intersex and hermaphrodite are no longer acceptable.
Sex Chromosome DSD
Turner’s syndrome
Turner’s syndrome is reported to occur in 1 in 2500 live female births [25]. There is complete or partial absence of the sex chromosome – most have the karyotype 45,XO, but 15% have a 46,XX mosaic pattern, and 7–10% have some Y chromatin present. The ovaries, located in their normal anatomical positions, consist mainly of fibrous stroma and are termed streak gonads. Germ cells rarely survive meiosis, follicular formation usually fails, and the resulting streak gonads are sterile and devoid of endocrine activity. At birth the genital ducts and external genitalia are entirely female, although clitoral enlargement may occasionally be present. However, almost 25% of girls with Turner’s syndrome show some secondary sexual development, 2–5% menstruate due to some residual ovarian function, and rarely, can have spontaneous pregnancies [ 26], although these are high risk because of the associated cardiac complications. Patients with Turner’s syndrome are of short stature and exhibit a range of somatic abnormalities including webbing of the neck, coarctation of the aorta, and renal anomalies. There is also a predisposition to develop diabetes mellitus and other autoimmune diseases, particularly those affecting the thyroid [ 27]. Hormonal treatments are required, and these patients need multidisciplinary specialist management throughout life [ 28]. There is a reduced incidence of breast cancer, but increased risk of gonadoblastoma and endometrial cancers [ 29].
Читать дальшеИнтервал:
Закладка:
Похожие книги на «Ridley's The Vulva»
Представляем Вашему вниманию похожие книги на «Ridley's The Vulva» списком для выбора. Мы отобрали схожую по названию и смыслу литературу в надежде предоставить читателям больше вариантов отыскать новые, интересные, ещё непрочитанные произведения.
Обсуждение, отзывы о книге «Ridley's The Vulva» и просто собственные мнения читателей. Оставьте ваши комментарии, напишите, что Вы думаете о произведении, его смысле или главных героях. Укажите что конкретно понравилось, а что нет, и почему Вы так считаете.