Protocols for High-Risk Pregnancies
Здесь есть возможность читать онлайн «Protocols for High-Risk Pregnancies» — ознакомительный отрывок электронной книги совершенно бесплатно, а после прочтения отрывка купить полную версию. В некоторых случаях можно слушать аудио, скачать через торрент в формате fb2 и присутствует краткое содержание. Жанр: unrecognised, на английском языке. Описание произведения, (предисловие) а так же отзывы посетителей доступны на портале библиотеки ЛибКат.

- Название:Protocols for High-Risk Pregnancies
- Автор:
- Жанр:
- Год:неизвестен
- ISBN:нет данных
- Рейтинг книги:3 / 5. Голосов: 1
-
Избранное:Добавить в избранное
- Отзывы:
-
Ваша оценка:
Protocols for High-Risk Pregnancies: краткое содержание, описание и аннотация
Предлагаем к чтению аннотацию, описание, краткое содержание или предисловие (зависит от того, что написал сам автор книги «Protocols for High-Risk Pregnancies»). Если вы не нашли необходимую информацию о книге — напишите в комментариях, мы постараемся отыскать её.
has helped busy obstetricians keep pace with a constantly evolving field. Providing just-in-time content, its focus on protocols and guidelines helps organize medical thinking, avoid heuristic errors of omission and commission, and optimize maternal and fetal outcomes.
As with the prior six editions, the editors have once again assembled some of the world’s top obstetrical and medical experts. This seventh edition has also been expanded to include a number of new topics, including:
Protocols on opioid use, misuse and addition in pregnancy and postpartum Noninvasive prenatal diagnosis of aneuploidy Periconceptual genetic screening Expanded protocols on maternal valvular heart disease and cardiomyopathies Protocols on arboviruses, including Zika and malaria
will be an essential reference for obstetricians, medical students, general practitioners and all medical professionals who are seeking the most up-to-date information and guidance on high-risk pregnancies.
Protocols for High-Risk Pregnancies — читать онлайн ознакомительный отрывок
Ниже представлен текст книги, разбитый по страницам. Система сохранения места последней прочитанной страницы, позволяет с удобством читать онлайн бесплатно книгу «Protocols for High-Risk Pregnancies», без необходимости каждый раз заново искать на чём Вы остановились. Поставьте закладку, и сможете в любой момент перейти на страницу, на которой закончили чтение.
Интервал:
Закладка:
There are three primary fetal circulatory shunts that require closure after delivery for normal newborn cardiopulmonary transition to occur and for the subsequent adult circulation to be established. As mentioned above, the DV shunts blood from the umbilical vein toward the heart. The ductus arteriosus shunts approximately 90% of the blood in the main pulmonary artery to the descending aorta, leaving only 10% of pulmonary artery blood to reach the fetal lungs. The third shunt is the foramen ovale, which is maintained in a patent state in utero to allow the process of preferential streaming to occur from the right atrium to the left. Failure of any one of these shunts to close properly may result in adverse cardiopulmonary transition in the newborn.
Fetal growth restriction
Fetuses that fail to reach their genetically determined growth potential due to uteroplacental dysfunction may develop abnormal resistance to blood flow in the placenta. This abnormal resistance is due to numerous placental vascular abnormalities (poor villous capillarization, reduced number and branching of stem arteries, luminal reduction, and wall hypertrophy), which can be detected with Doppler velocimetry in the umbilical artery located upstream from the placenta. Progression of placental disease with concomitant worsening of blood flow resistance may lead to additional Doppler velocimetry changes in the central nervous system, and eventually in the precordial venous system or the heart. Once the fetus decompensates to that level of Doppler abnormality, acidemia is nearly always present.
Fetal anemia
In Rh disease, a fetal RBC antigen enters the maternal bloodstream and stimulates antibody production against that RBC antigen. An amnestic response may occur in a subsequent pregnancy if the same RBC antigen is presented to the mother’s immune system and this may lead to a series of events that include fetal anemia, extramedullary hematopoiesis, hydrops fetalis, and fetal death. Historically, the degree of fetal anemia and need for fetal RBC transfusion involved an amniocentesis to determine the amniotic fluid ΔOD450 to assess the degree of RBC‐derived hemoglobin breakdown products and to estimate anemia. Isoimmunization with the Kell antibody also results in fetal anemia but does so through bone marrow suppression rather than hemolysis and thus, the ΔOD450 will not be abnormal. Fetal anemia can also result from infections such as parvovirus B19. Doppler velocimetry of the middle cerebral artery (MCA) is now used to determine the risk for moderate to severe anemia supplanting the previously used amniocentesis. If moderate to severe anemia is suspected, the fetus should undergo a fetal blood sampling and transfusion.
Preterm labor
Although the pathophysiology of preterm labor is still largely unknown, tocolytic use is widespread. Use of agents that inhibit prostaglandin synthesis can result in premature closure of the ductus arteriosus and oligohydramnios. Doppler velocimetry is useful in assessment of ductus arteriosus closure by determining the peak systolic velocity as well as whether there is continuous flow throughout diastole.
Cardiac abnormalities
Fetuses with known cardiac abnormalities including congenital or structural heart disease, arrhythmias and congestive failure may have intracardiac and outflow tract flow velocity abnormalities that can be detected with Doppler velocimetry. Depending on the nature of the abnormality, this can affect other flow velocity waveforms including the DV, hepatic veins, inferior vena cava, and umbilical vein.
Diagnosis
Doppler techniques and measurements
As mentioned in the overview, pulse‐wave Doppler velocimetry can be used to obtain the following information from a flow velocity waveform.
Velocity of the blood – requires an angle of insonation of zero degrees between the transducer and the vessel of interest ( Figure 7.1). The angle correction function available on most ultrasound machines can be used but the actual angle between the vessel and the ultrasound beam should be less than 30°. For middle cerebral artery peak systolic velocity (MCA PSV), the sample volume should be placed in the proximal third of the MCA as it branches from the circle of Willis.
Resistance indices (systolic/diastolic or S/D ratio, resistance index, pulsatility index) – these are angle‐independent measurements such that the value obtained for any one of these indices is not dependent upon the angle between the transducer and the vessel being interrogated ( Figure 7.2).
Volume blood flow (milliliters per minute) – this is determined by obtaining the velocity of the blood and multiplying it by the cross‐sectional area of the vessel (obtained by two‐dimensional ultrasound) times 60 seconds:
Volume flow (mL/min) = velocity (cm/sec) × cross‐sectional area (cm2) × 60 seconds
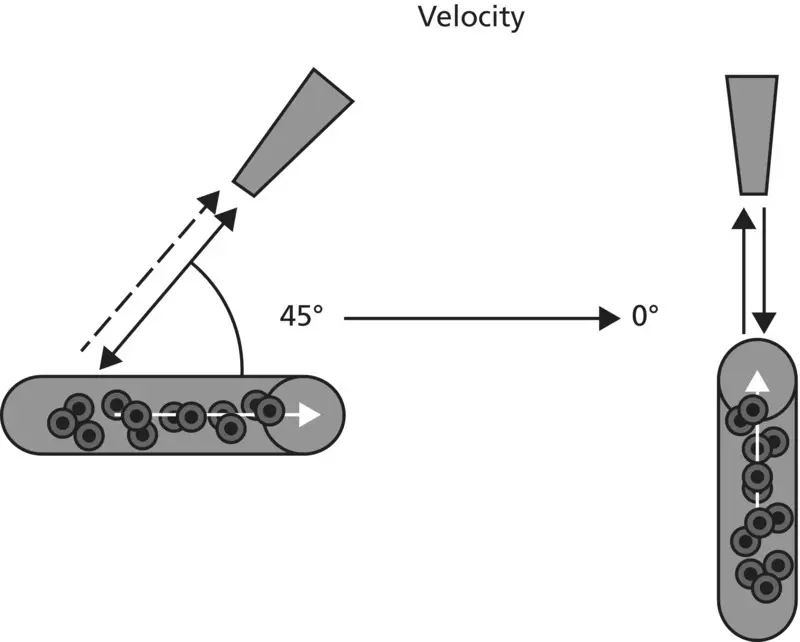
Figure 7.1 Schematic representing zero angle of insonation between the Doppler transducer and the vessel of interest.
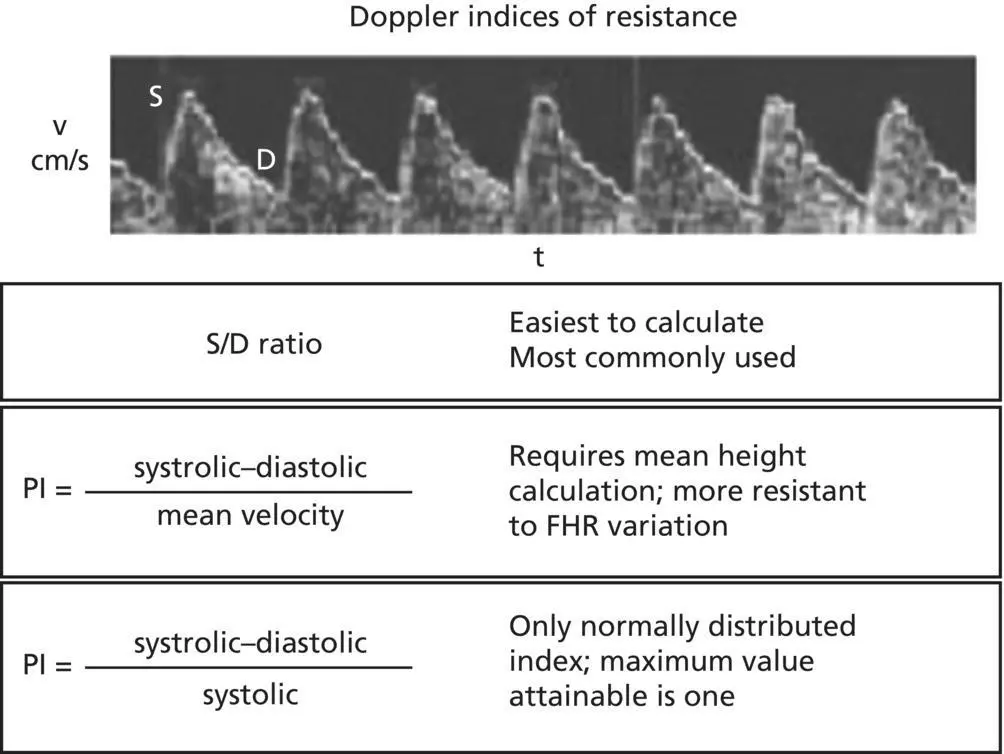
Figure 7.2 Flow velocity waveform of the umbilical artery and definitions for the different Doppler indices of resistance.
Cardiac flow velocities
Normal values and blood flow velocity patterns have been previously reported for cardiac Doppler velocities. More specifically, blood flow velocity values and patterns have been described for the pulmonary and aortic outflow tracts, ductus arteriosus, DV, pulmonary veins, tricuspid and mitral valve, and inferior vena cava. Any fetal structural cardiac abnormality or precordial or postcordial vascular abnormality can affect the blood flow velocity and waveform of the aforementioned vessels and valves. Further discussion of fetal echocardiography is found in Protocol 6.
Prediction of adverse pregnancy events
There has been considerable effort over the past two decades with the application of maternal Doppler studies of the uterine arteries in the prediction of adverse pregnancy outcomes including preeclampsia, FGR, fetal demise, and preterm birth. The most distal branches of the uterine artery (spiral arteries) undergo a remarkable transition during the first half of pregnancy, from highly muscularized vessels with high resistance to remodeled vessels with low resistance. This is in response to differentiation of cytotrophoblast to noninvasive and invasive cytotrophoblast, with the latter literally invading and altering spiral artery muscular architecture. It is this change that leads to the enormous blood flow eventually seen in pregnancy (600–800 mL/min).
There are many publications on the use of uterine artery Doppler for predicting adverse pregnancy outcomes in both low‐risk and high‐risk populations. In the low‐risk population, there does not seem to be a benefit of wide application of this Doppler test as a screening tool for adverse pregnancy events. There may be a role in uterine artery Doppler testing in high‐risk pregnancy as it may identify a subgroup of patients at a higher risk for adverse events, which may lead to useful additional monitoring during pregnancy or preventive strategies. In addition, the high negative predictive value for adverse pregnancy events can provide reassurance. However, before this test can be applied to the general or even the high‐risk pregnancy population, further evidence is needed to elucidate a clear predictive capability, the optimum gestational age for screening, standardization for study technique and abnormal test criteria, and an effective prevention therapy or strategy; this position has been supported by the Society for Maternal‐Fetal Medicine.
Читать дальшеИнтервал:
Закладка:
Похожие книги на «Protocols for High-Risk Pregnancies»
Представляем Вашему вниманию похожие книги на «Protocols for High-Risk Pregnancies» списком для выбора. Мы отобрали схожую по названию и смыслу литературу в надежде предоставить читателям больше вариантов отыскать новые, интересные, ещё непрочитанные произведения.












Обсуждение, отзывы о книге «Protocols for High-Risk Pregnancies» и просто собственные мнения читателей. Оставьте ваши комментарии, напишите, что Вы думаете о произведении, его смысле или главных героях. Укажите что конкретно понравилось, а что нет, и почему Вы так считаете.