Richard J. Banchs - The Quality Improvement Challenge
Здесь есть возможность читать онлайн «Richard J. Banchs - The Quality Improvement Challenge» — ознакомительный отрывок электронной книги совершенно бесплатно, а после прочтения отрывка купить полную версию. В некоторых случаях можно слушать аудио, скачать через торрент в формате fb2 и присутствует краткое содержание. Жанр: unrecognised, на английском языке. Описание произведения, (предисловие) а так же отзывы посетителей доступны на портале библиотеки ЛибКат.
- Название:The Quality Improvement Challenge
- Автор:
- Жанр:
- Год:неизвестен
- ISBN:нет данных
- Рейтинг книги:5 / 5. Голосов: 1
-
Избранное:Добавить в избранное
- Отзывы:
-
Ваша оценка:
The Quality Improvement Challenge: краткое содержание, описание и аннотация
Предлагаем к чтению аннотацию, описание, краткое содержание или предисловие (зависит от того, что написал сам автор книги «The Quality Improvement Challenge»). Если вы не нашли необходимую информацию о книге — напишите в комментариях, мы постараемся отыскать её.
equips readers with the skills and knowledge required to develop and implement successful operational improvement initiatives.
Designed for healthcare providers seeking to apply QI in practice, this valuable resource delivers step-by-step guidance on improvement methodology, team dynamics, and organizational change management in the context of real-world healthcare environments. The text integrates the principles and practices of Lean Six Sigma, human-centered design, and neurosciences to present a field-tested framework. Detailed yet accessible chapters cover topics including identifying and prioritizing the problem, developing improvement ideas, defining the scope of the project, organizing the QI team, implementing and sustaining the improvement, and much more. Clearly explaining each step of the improvement process, this practical guide:
Presents the material in a logical sequence, gradually introducing each step of the process with clearly defined workflow templates Features a wealth of examples demonstrating QI application, and case studies emphasizing key concepts to highlight successful and unsuccessful improvement initiatives Includes end-of-chapter exercises and review questions for assessing and reinforcing comprehension Offers practical tips and advice on communicating effectively, leading a team meeting, conducting a tollgate review, and motivating people to change Leading QI projects requires a specific set of skills not taught in medical school.
bridges this gap
for
experienced and trainee healthcare providers, and serves as an important reference for residency program directors, physician educators, healthcare leaders, and health-related professional organizations.
The Quality Improvement Challenge — читать онлайн ознакомительный отрывок
Ниже представлен текст книги, разбитый по страницам. Система сохранения места последней прочитанной страницы, позволяет с удобством читать онлайн бесплатно книгу «The Quality Improvement Challenge», без необходимости каждый раз заново искать на чём Вы остановились. Поставьте закладку, и сможете в любой момент перейти на страницу, на которой закончили чтение.
Интервал:
Закладка:
Scan the environment, listen to people, and observe the work environment around you. Start by asking yourself these four questions:
1 What is important to my patients? What are their needs and expectations? What do they want from the care we provide? Where does our performance fall short?
2 What are the needs of providers and staff? What do they need to succeed? What are their challenges? What are their “pain points”?
3 What is my area struggling with? What are the issues affecting us (unit or department)? What are the strategic initiatives planned for this year? Where do we fall short in our performance?
4 What is my hospital struggling with? What are some of the hospital’s strategic initiatives, and how do these translate to my daily work? What issues affect our hospital (healthcare organization)?
The answer to these and other questions may give you an insight into what improvements are most urgently needed. Sometimes a quality improvement (QI) project idea may come from your own daily experience. What are you struggling with? What are the challenges and barriers that prevent you from doing your work? What can be improved in your work environment?
Your personal experience, the needs of your patients, and challenges of the frontline staff and providers are all sources of project ideas. If you are a healthcare leader, all ideas should be considered: top‐down from supervisors and leaders and bottom‐up from providers and frontline staff. Anyone should be able to suggest an improvement idea. Timely, constructive feedback should be provided by leaders to those who forward an improvement idea, regardless of the final decision to move ahead with a QI project.
Consider the Three “Voices” for Project Ideas
In general, project ideas come from three sources. We call them the voices. They are the “Voice of the Customer,” the “Voice of the Stakeholder,” and the “Voice of the Process” (see Figure 3‐1).
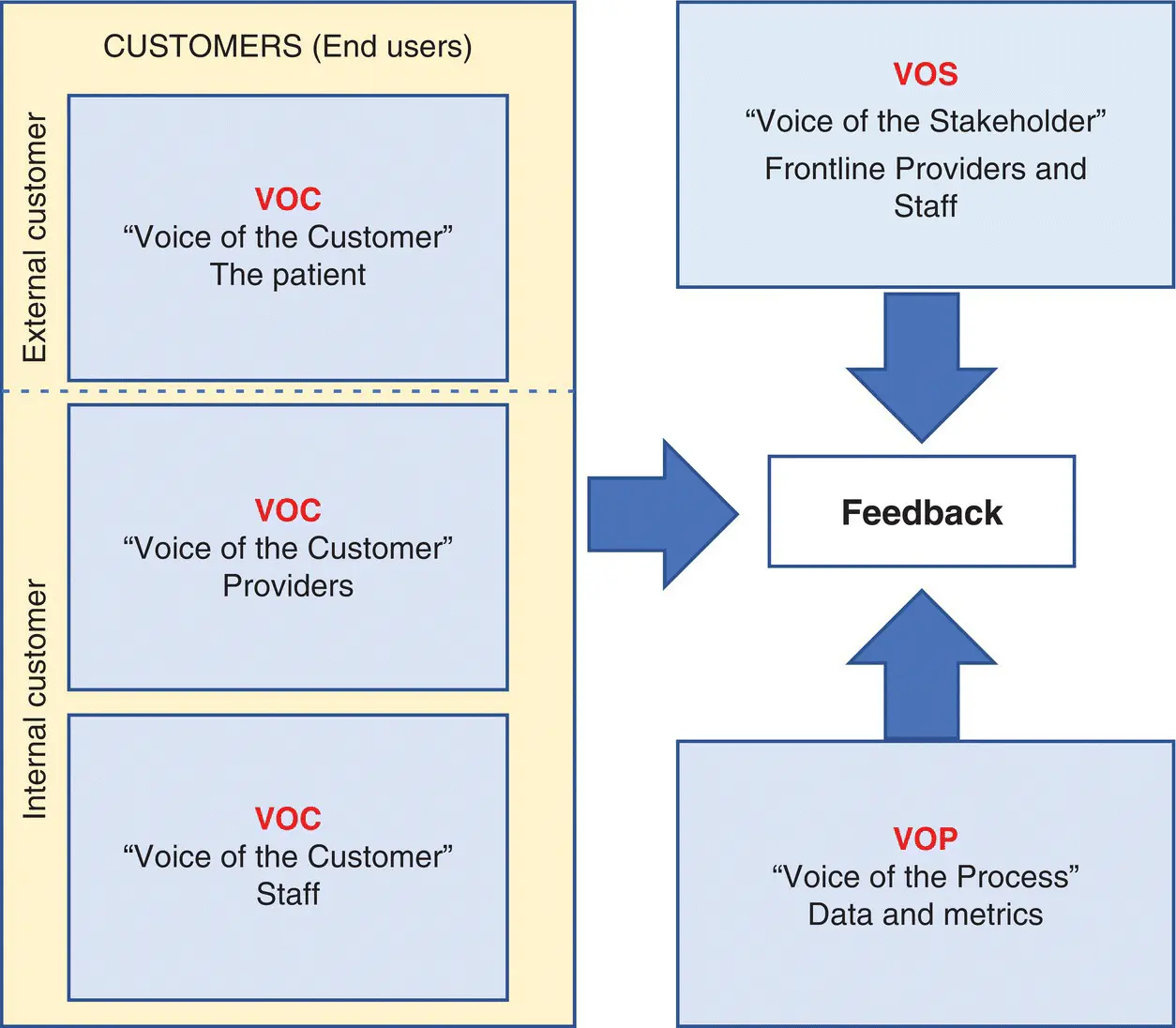
FIGURE 3‐1Three main sources for project ideas.
The Voice of the Customer (VOC)
The VOC is the expression of the needs and expectations of the customers . In healthcare, patients are our “customers,” and their needs and expectations should drive our QI efforts. However, as in healthcare, most organizations have two types of customers:
1 External customers. These are our patients. We launch improvement projects to address their needs, concerns, and expectations. When we listen to our patients at the point‐of‐care, review patient surveys, or speak to their families we may find patients’ expectations are not met. We may then ask ourselves, how can we improve the care we provide and make their experience a better one?
2 Internal customers. The internal customers are the staff and providers at the front line. Sometimes the customer is not the patient. Frontline staff and providers depend on others for the work they do. They are the end users. Clinical practice involves caring for patients. But to care for patients, providers and staff need consultations, diagnostic imaging, lab work, demographic and insurance information, nutritional services, and so on. Providers and staff provide services to patients, but in turn depend on other providers and staff for their work. When these providers and staff receive the work product of other providers and staff, we call them customers. The providers and staff that perform services for other providers and staff are called stakeholders. Stakeholders are the professionals “doing the work.” Improvement initiatives sometimes are needed to improve the work products our internal customers receive. Example: When you, as a provider, order a chest X‐ray, you are the “customer,” not the patient. The patient will benefit from the treatment approach you prescribe and is the ultimate and last customer. But for the chest X‐ray, you are the customer. What will happen if the radiology technician routinely takes an hour to show up? What if the official reading of a STAT chest X‐ray takes a day? What if a large number of chest X‐rays are overpenetrated, underpenetrated, or miss the costo‐phrenic angle? You, the customer, will not be happy (and rightfully so!). Based on the VOC (internal customer), the radiology department may decide to initiate a QI project.
The Voice of the Stakeholder (VOS)
The VOS is the expression of the needs and requirements of the frontline professionals . Stakeholders are the frontline staff and providers; they are the people “doing the work”; they are the professionals with the subject‐matter expertise and knowledge of the process. Stakeholders understand the system and are the experts needed for the process to deliver what the customer needs and expects . Stakeholders may be staff, physicians, nurses, or technicians involved in providing care. Stakeholders work on the process to provide a work product. When serving patients, the work product is “care and the healthcare experience”; when serving other providers and staff, the work product may be “information, supplies, results, etc.”
Stakeholders want to do a good job. To perform optimally, they need equipment, supplies, information, and resources, on time, every time. They also need standards, updated policies, and proper procedures. If there is a problem with their performance, we need to ask ourselves: Do they have what they need? What are their challenges? Stakeholders’ inability to deliver the service the customer needs and expects may be related to problems with the system: Do needed supplies arrive on time? Is the equipment in working condition? Is the work process standardized? Perhaps frontline stakeholders don’t have the equipment and supplies they need, or the people responsible for supplying them with what they need are not doing so in a timely fashion. In any case, a QI project may need to be launched to find the causes of poor performance and address stakeholders’ needs.
The Voice of the Process (VOP)
The VOP is how the process communicates performance against customer needs and expectations . This communication is done through process measures and in the form of data. Sometimes a QI project is launched to address process performance on a specific metric. This is the case when financial reports, clinical audits, and other types of data show a gap in performance. There may be an increased number of complications or readmission rates. Even if we don’t have a VOC or VOS, the VOP (increased costs, slow response times, miscoded charts, increased narcotic discrepancies in the MICU, etc.) may be reasons why you and your team decide to launch a QI project.
Quotable quote: “If opportunity doesn’t knock, build a door.” Milton Berle
THE PROJECT SELECTION PROCESS
The Goal
The goal of the Project Selection Process is to select a QI project that is important to you and your organization in addressing critical issues of patient care, healthcare experience, costs, and resource utilization. A weak, undefined Project Selection Process makes improvement efforts more difficult and time consuming. A strong, defined, communicated and ingrained Project Selection Process can really make a significant difference in a healthcare organization’s improvement efforts. A strong project selection process has the following characteristics:
Projects are selected from both leadership and the front line (top down and bottom up); anyone can initiate a project idea.
Читать дальшеИнтервал:
Закладка:
Похожие книги на «The Quality Improvement Challenge»
Представляем Вашему вниманию похожие книги на «The Quality Improvement Challenge» списком для выбора. Мы отобрали схожую по названию и смыслу литературу в надежде предоставить читателям больше вариантов отыскать новые, интересные, ещё непрочитанные произведения.





Обсуждение, отзывы о книге «The Quality Improvement Challenge» и просто собственные мнения читателей. Оставьте ваши комментарии, напишите, что Вы думаете о произведении, его смысле или главных героях. Укажите что конкретно понравилось, а что нет, и почему Вы так считаете.