Smart Healthcare System Design
Здесь есть возможность читать онлайн «Smart Healthcare System Design» — ознакомительный отрывок электронной книги совершенно бесплатно, а после прочтения отрывка купить полную версию. В некоторых случаях можно слушать аудио, скачать через торрент в формате fb2 и присутствует краткое содержание. Жанр: unrecognised, на английском языке. Описание произведения, (предисловие) а так же отзывы посетителей доступны на портале библиотеки ЛибКат.
- Название:Smart Healthcare System Design
- Автор:
- Жанр:
- Год:неизвестен
- ISBN:нет данных
- Рейтинг книги:4 / 5. Голосов: 1
-
Избранное:Добавить в избранное
- Отзывы:
-
Ваша оценка:
Smart Healthcare System Design: краткое содержание, описание и аннотация
Предлагаем к чтению аннотацию, описание, краткое содержание или предисловие (зависит от того, что написал сам автор книги «Smart Healthcare System Design»). Если вы не нашли необходимую информацию о книге — напишите в комментариях, мы постараемся отыскать её.
Smart Healthcare System: Security and Privacy Aspects
Smart Healthcare System Design — читать онлайн ознакомительный отрывок
Ниже представлен текст книги, разбитый по страницам. Система сохранения места последней прочитанной страницы, позволяет с удобством читать онлайн бесплатно книгу «Smart Healthcare System Design», без необходимости каждый раз заново искать на чём Вы остановились. Поставьте закладку, и сможете в любой момент перейти на страницу, на которой закончили чтение.
Интервал:
Закладка:
2.4.3 An Issue With the Tele-Medication
Monitoring and mobility of ambulatory patients can cause of late delivery of tele-medication at a patient location. In the case of any abnormality, the tele-medication has to reach the location at the right time. This tele-medication is mostly sent by the associated doctor, who is monitoring the patient. If the distance of the doctor and patient is too far from each other then it can cause the critical condition of the patient. Therefore, tele-medication is very important to reach the patient location but is still an issue in cardiac patient monitoring for smart health. The research community has done work related to the mortality rate due to issue with the tele-medication. In the study of [36] it mentioned that the mortality rate is quite high after some surgical treatment in patients due to unreachability of tele-medication services at the patient’s end. The rate of mortality rose from 7–9.5% due to this issue. In another study [35] reported that due to less effective services of tele-medication to mobile patients the rate of mortality becomes high. After the treatment patients can get a short-term indicative improvement in their health. But after the discharge from the hospital, the death rate becomes high within the first year due to unreachable tele-medication services, less qualitative monitoring, and readmission of patients in the case of any abnormality. In certain instances, the death rate and readmission are very high as the ‘vulnerable stage’ is called the 1st months after hospitalization to recognize hospitalization. The danger of death and readmission is usually evident during the 1–3 months following the release of the crisis center, with the highest rates occurring in the initial 30 days. Information from the US ADHERE library, considering 104,808 patients hospitalized inferable from HF, tended to have 11.2% mortality data and a 22.1% readmission rate on Day 30 after release. Some 35–40% of patients will either send or be readmitted to an emergency clinic during the baseline 3 months after discharge. In the primary year after hospitalization for HF, syphon dissatisfaction and sudden cardiovascular passing are the most normal purposes behind death. The general photo, as Figure 2.2below, expresses that situation.
This study also examined the death rate of outpatients due to less intelligent tele-medication services offered. The study stated that the visits of patients after the treatment were good after the post-discharge, but steadily decreased as days passed. Therefore, ambulatory patients need a smart tele-medication definition to track and take appropriate action when any abnormality occurs. As shown in the figure below the median period from entry to an initial portion of the sample was 7 days in the pre-release collection and 10 days in the post-release collection. In separate pre-release and post-release meetings, the median period from randomization to the primary component was 0 days [interquartile run (IQR) 0–1 days] and 3 days (IQR 2–6 days). In the pre-release gathering (IQR −2 to −1 days) and 1 day in the post-release gathering (IQR 1–4 days), the median time from release to the main component was −1 day as illustrated in Figure 2.3.
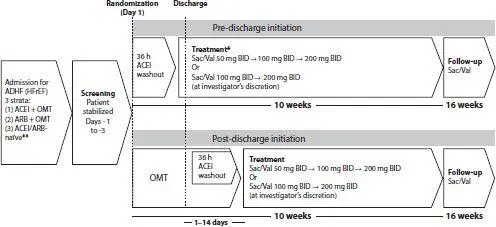
Figure 2.2 Structure of transformation research. Visits to the study occur at 2, 4, 6, 8, and 10 weeks and 14, 18, 22, and 26 weeks after randomization (or at the time of early treatment or suspension of the study) [35]. ACEI, angiotensin-changing chemical inhibitor; ADHF, extreme decompensated cardiovascular failure; ARB, angiotensin receptor blocker; HFrEF, reduced discharge cardiovascular failure; OMT, advanced medical clinical treatment; Sac/Val, sacubitril/valsartan [49].
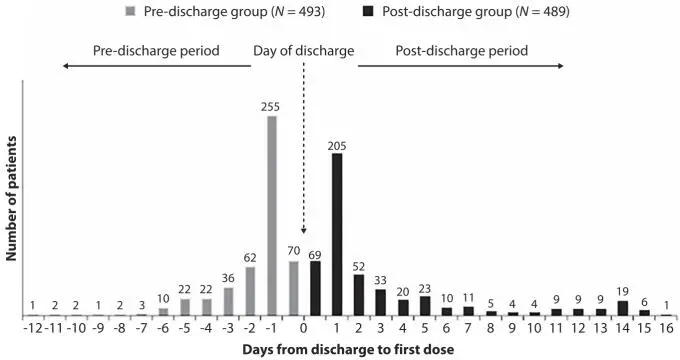
Figure 2.3 The no. of patients visits after Post Discharge [36].
2.4.4 Mobility of Doctor
There is also an issue with the mobility of a doctor rather than the patient mobility. The specified monitoring doctor can also be in a mobile state and when the abnormality occurs with the patient, might be the doctor does not know about it. The mobility of health professionals (doctors, paramedical staff) can cause a critical situation for patients in the case of any abnormality. As stated in the study that the healthcare professionals move from place to place just due to some benefits. Due to their mobility to other places the patients face different issues that need serious attention from the policymakers. The study reported that some patients need care at their geographical locations [48, 50].
2.4.5 Application User Interface Issue
Numerous applications are created by the planner and designers yet all applications have a few restrictions because of the innovation and situations change around patients. The UI oversees issues, for instance, graphical UI (sensors affiliation control, menu, sounds and voice messages, the status of the system, a demonstration of data, etc.), speaker, keys, drove, and other device limits like vibration. This issue generally happens in versatile wellbeing situations, where the wellbeing portable application configuration isn’t easy to understand for patients. One of the essential challenges of flexible prosperity is using the humbler screens of mobile phones successfully to show information supporting the prosperity dynamic system. Along these lines, it is imperative to discover proficient ways of utilizing the screens of cell phones to show important data supporting dynamic [49].
2.5 Security Threats
The idea of s-Health and all the applications and frameworks that could lie inside could fundamentally push residents to improve their personal satisfaction and medicinal services administrations while the expenses of the human services framework are decreased. In the situation that we talked about in the past segment, s-Health uses the frameworks and ICT of the city to furnish preventive strategies to residents with respiratory conditions. Consequently, such residents could all the more likely control their sickness and diminish costs on the medicinal services framework. Notwithstanding, there might be some potential security issues in this engineering. Residents may not need to be completely observed. Also, taking into account the dispersed and remote nature of sensor systems, guaranteeing information security is an incredible test for s-Health frameworks. Too, because of the very idea of s-Health frameworks (i.e., profoundly dispersed, remote), it is difficult to incorporate a security control in contrast with conventional human services frameworks. Furthermore, listening to stealthily and skimming happen when the sensor information is transmitted through remote systems. There are many security issues with the health-related data as the health record of the patient is stored either on single or multiple servers [51–53]. The security breaches with the data are as follows.
2.5.1 Identity Privacy
Character security with regards to s-Health identifies with ensuring the personality of residents that get to s-Health administrations. The eHealth framework and other specialist co-ops can utilize the character of a patient to connect their exercises or his/her wellbeing condition and records. In our design, when a resident contacts the CCC, his/her personality is presented to the outside. Residents’ personalities can be unlawfully utilized by programmers to get touchy individual data in the focal database, for example, electronic wellbeing records and arrangements of areas. Accordingly, protection could be attacked. This is one of the principal issues among all protection issues. To address this issue, most arrangements depend on halfway substances to conceal the genuine personalities of the clients (e.g., utilizing nom de plumes). Additionally, because of a coordinated effort among clients, the creators proposed utilizing (confided in outsider)based methodologies. By and by, the personality is still at serious risk if the CCC is enduring an onslaught or the supervisors of the administrations get out of hand. To maintain a strategic distance from this circumstance, we think about that as a lot of topographically disseminated pseudonymized are required.
Читать дальшеИнтервал:
Закладка:
Похожие книги на «Smart Healthcare System Design»
Представляем Вашему вниманию похожие книги на «Smart Healthcare System Design» списком для выбора. Мы отобрали схожую по названию и смыслу литературу в надежде предоставить читателям больше вариантов отыскать новые, интересные, ещё непрочитанные произведения.






Обсуждение, отзывы о книге «Smart Healthcare System Design» и просто собственные мнения читателей. Оставьте ваши комментарии, напишите, что Вы думаете о произведении, его смысле или главных героях. Укажите что конкретно понравилось, а что нет, и почему Вы так считаете.