Manual of Equine Anesthesia and Analgesia
Здесь есть возможность читать онлайн «Manual of Equine Anesthesia and Analgesia» — ознакомительный отрывок электронной книги совершенно бесплатно, а после прочтения отрывка купить полную версию. В некоторых случаях можно слушать аудио, скачать через торрент в формате fb2 и присутствует краткое содержание. Жанр: unrecognised, на английском языке. Описание произведения, (предисловие) а так же отзывы посетителей доступны на портале библиотеки ЛибКат.
- Название:Manual of Equine Anesthesia and Analgesia
- Автор:
- Жанр:
- Год:неизвестен
- ISBN:нет данных
- Рейтинг книги:3 / 5. Голосов: 1
-
Избранное:Добавить в избранное
- Отзывы:
-
Ваша оценка:
Manual of Equine Anesthesia and Analgesia: краткое содержание, описание и аннотация
Предлагаем к чтению аннотацию, описание, краткое содержание или предисловие (зависит от того, что написал сам автор книги «Manual of Equine Anesthesia and Analgesia»). Если вы не нашли необходимую информацию о книге — напишите в комментариях, мы постараемся отыскать её.
Provides practical, clinically oriented information on anesthetizing equids Uses a bulleted format designed for fast access of key information Offers step-by-step instructions and diagrams of nerve blocks of the limbs, head, and ophthalmic structures Includes new coverage of topics including regulation of extracellular fluid and blood pressure, acid-base disorders, and hemodynamic effects of autonomic drugs
remains a must-have resource for all equine practitioners and veterinary students involved with anesthetizing horses.
Manual of Equine Anesthesia and Analgesia — читать онлайн ознакомительный отрывок
Ниже представлен текст книги, разбитый по страницам. Система сохранения места последней прочитанной страницы, позволяет с удобством читать онлайн бесплатно книгу «Manual of Equine Anesthesia and Analgesia», без необходимости каждый раз заново искать на чём Вы остановились. Поставьте закладку, и сможете в любой момент перейти на страницу, на которой закончили чтение.
Интервал:
Закладка:
Source: Courtesy of: Dr. Peter Rakestraw, VMD, Dip ACVS.
II Indications
To bypass an obstruction of airflow proximal to the site of tracheostomy. The horse is an obligate nasal breather, so severe obstruction of the nasal cavity necessitates creating a tracheostomy.
To provide access to the trachea for administering an inhalant anesthetic and oxygen, so that surgery of the larynx or pharynx (e.g. resection of the nasal septum, arytenoidectomy, repair of a cleft palate) can proceed unimpeded by the presence of an ET tube.
III Surgical anatomy
Structures overlying the site of tracheostomy include the skin and cutaneous coli, sternohyoideus, and thyrohyoideus muscles.
The site of tracheal incision is the annular ligament of the trachea, which attaches one tracheal ring to another.
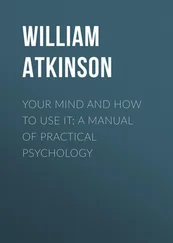
IV Tracheostomy tubes (see Figure 4.12)
J‐type tube.
Dyson tube (self‐retaining).
Bivona silicone tube.
A temporary tracheostomy tube can be made, in an emergency, from the handle of a one‐gallon plastic jug or the cut end of a large stomach tube or garden hose.

Figure 4.12 Tracheostomy tubes: Bivona silicon tube (a), Dyson tube (b), a tube made from a gallon plastic jug (c), and a J‐type tube (d).
V Technique
Tracheostomy is usually performed with the horse standing, but can also be performed under general anesthesia in anticipation of a post‐surgical obstruction.
The procedure is performed most easily with the horse restrained in stocks and sedated with an alpha2 agonist, such as detomidine HCl (0.005–0.01 mg/kg, IV) or xylazine HCl (0.2–0.5 mg/kg, IV)Butorphanol tartrate (0.02–0.03 mg/kg, IV) can be administered after the horse is sedated, if necessary, to provide more profound sedation.
The usual site is the juncture of the cranial and middle third of the cervical portion of the trachea (3rd to 6th tracheal rings).The trachea can usually be palpated easily at this site.If the surgeon anticipates that the horse may later require a permanent tracheostomy, the site of temporary tracheostomy should be far enough distal on the neck that it does not interfere with creating a permanent tracheostomy.
Hair at the proposed site of incision is clipped, and the site is scrubbed.
8–12 ml of local anesthetic solution is injected subcutaneously at the proposed site of incision (see Figure 4.13).
A 5–9 cm, longitudinal incision is made through the skin, subcutaneous tissue, and cutaneous coli muscle (see Figure 4.14).
The juncture between the right and left sternohyoideus muscles and the right and left sternothyroideus is incised with a scalpel or scissors. Finding the site of the juncture is often difficult and not absolutely necessary.Avoid inadvertently scoring the tracheal rings when the musculature is incised with a scalpel.
Retracting the skin and musculature with a Weitlaner or Gelpi retractor helps to expose the trachea (see Figure 4.15).Inserting a retractor into the wound can be omitted if the tracheostomy is being performed with urgency. Figure 4.13 Local anesthetic is instilled subcutaneously at the proposed site of incision in preparation for performing a temporary tracheostomy. Figure 4.14 A cutaneous incision is created on the ventral midline of the neck over the palpable trachea. This incision is extended through the cutaneous colli and the right and left sternothyroideus muscles to expose the tracheal rings. Figure 4.15 The trachea can be better exposed by separating the cutaneous and muscular incision with a self‐retaining retractor.
The annular ligament between two tracheal rings is identified in the center of the incision, and this ligament is incised with a scalpel blade to expose the lumen of the trachea, being careful to avoid inadvertently incising the mucosa on the dorsal side of the trachea.The ligament and underlying tracheal mucosa are incised to the right or left, and without removing the blade from the incision, the blade is turned over, and the incision is lengthened in the other direction.Ideally, the tracheal incision should be approximately one‐third of the circumference of the trachea if a tracheostomy tube is to be inserted. The incision needs to be larger, if it is created for insertion of an endotracheal tube through which an inhalant anesthetic and oxygen are to be administered.The tracheal incision should not exceed half of the tracheal circumference.Extending the incision beyond one‐half of the circumference risks formation of a restrictive cicatrix and transection of an adjacent carotid artery or a nerve, such as the vagosympathetic trunk or recurrent laryngeal nerve, which lies adjacent to the carotid artery.Note: The scalpel blade should be attached to a scalpel handle, if time allows, so that inadvertent loss of the blade into the lumen of the trachea is avoided.Incision into the tracheal lumen can be recognized by escape of air through the wound when the horse exhales. The horse may cough, because of blood entering the tracheal lumen.
A finger or the jaws of a large forceps are inserted into the lumen of the trachea, through the incised annular ligament and tracheal mucosa, and the cannula of a tracheostomy tube is inserted between the two separated tracheal rings, adjacent to the finger or jaws of the opened forceps, into the lumen of the trachea.
The tracheostomy tube is secured to the site of tracheostomy. Each side of the faceplate (or neck flange) of a J‐tube has a slot through which rolled gauze can be threaded and tied around the neck.To ensure that a J‐tube does not become dislodged, it can be sutured to the neck through the slot on each side of the faceplate or secured to the neck with elastic adhesive tape.Dyson tubes are self‐retaining and need not be secured.
To ease replacing the tube, a long suture can be placed around each ring adjacent to the tracheal incision. Traction on these sutures widens the tracheal incision for easy insertion of the cannula of the tube and prevents the cannula of the tube from being inserted subcutaneously.The cannula is easily replaced, without the use of sutures, after the wound has developed granulation tissue, usually by day 6.
Some clinicians, when anticipating a lengthy period of tracheal cannulation, such as for maintaining a tracheal stoma for a working season, remove a crescent‐shaped section of cartilage from the distal aspect of the ring proximal to the incision in the annular ligament, and a similar section from the proximal aspect of the ring distal to the incision in the annular ligament (see Figure 4.16).Although removing sections of cartilage may ease daily insertion of the tracheostomy tube, removing cartilage is seldom necessary.
VI Post‐operative care
The horse should be administered a tetanus toxoid vaccination, if it has not received one within the previous year.It should be administered a tetanus toxoid vaccination and tetanus antitoxin if it has never been vaccinated against tetanus.
The horse should be administered a broad‐spectrum antibiotic until the tracheal wound begins to develop granulation tissue, usually at five to six days.
Compressing the tissue at the site of tracheostomy by securing the tracheostomy tube with an elastic adhesive bandage applied around the neck and faceplate, leaving the entrance to the cannula uncovered, may decrease the severity of subcutaneous emphysema, which frequently develops at the site. Figure 4.16 To ease daily insertion of a tracheostomy tube, a crescent‐shaped section of cartilage can be excised from the distal aspect of the ring proximal to the incision through the annular ligament of the trachea, and a similarly shaped section of cartilage can be removed from the proximal aspect of the adjacent ring.Source: Courtesy of Dr. Peter Rakestraw, VMD, Dip ACVS. Figure 4.17 Compressing the faceplate of the tracheostomy tube against the tracheal incision diminishes the likelihood of the horse developing excessive subcutaneous emphysema adjacent to the incision.
Читать дальшеИнтервал:
Закладка:
Похожие книги на «Manual of Equine Anesthesia and Analgesia»
Представляем Вашему вниманию похожие книги на «Manual of Equine Anesthesia and Analgesia» списком для выбора. Мы отобрали схожую по названию и смыслу литературу в надежде предоставить читателям больше вариантов отыскать новые, интересные, ещё непрочитанные произведения.




Обсуждение, отзывы о книге «Manual of Equine Anesthesia and Analgesia» и просто собственные мнения читателей. Оставьте ваши комментарии, напишите, что Вы думаете о произведении, его смысле или главных героях. Укажите что конкретно понравилось, а что нет, и почему Вы так считаете.